


Abstract
Despite the widely demonstrated public health benefits of contraception, limited contraceptive options are available for men, placing both the contraceptive burden and opportunity solely on women. This review outlines the need for an increased focus on male contraceptive development and highlights several related topics, including the perspectives of women and men on male contraceptives, historical challenges, and reasons behind the persistent delays in male contraceptive development. It also discusses the importance of serendipitous observations in drug discovery and the limitations of depleting sperm or spermatogenic cells as a contraceptive approach. It further provides an overview of ongoing research and development on novel methods, with a goal to offer insights into the multifaceted aspects of nonhormonal male contraceptive development, addressing its implications for the health of men and women.
Significance Statement Despite well over half a century of effort in developing male contraceptives, there are no approved male contraceptive drugs on the market. This review aims to present strategies for progress in nonhormonal male contraception based on lessons learned from history, with the hope of expediting development and bringing a male contraceptive drug closer to reality.
I. Male Contraceptive Development Is, After All, a Women’s Health Issue
Since the advent of the condom sometime prior to the 18th century and the popularization of vasectomy as a sterilization procedure in the 1900s, no novel contraceptive options have been introduced for men, either pharmacological or otherwise (Sheynkin, 2009; Amy and Thiery, 2015). New contraceptive methods have almost exclusively favored options for women, and innovations have largely centered around the method of administration and access to existing hormonal active pharmaceutical ingredients, rather than the generation and introduction of new compounds. This means that the contraceptive method mix has grown to contain contraceptive products with a wide range of means of administration but with a focus on only a subset of the population and a single mechanism of action. As unintended pregnancy remains one of the most pervasive global health crises with nearly half of all pregnancies unintended each year, it remains critical that we enhance our focus on providing new contraceptive tools for users, particularly men, a group that remains underserved and underrepresented in family planning (Hardee et al., 2017; Jacobstein et al., 2023). (Note that this review for the purposes of clarity interchangeably uses gendered terminology such as “male,” “female,” “men,” and “women” but is cognizant of the need to consider nonbinary and other nonconforming users in the development of these methods.)
The 213 million global unintended pregnancies each year (The-Guttmacher-Institute, 2022) are associated with a myriad of negative outcomes for pregnant people and their offspring that go above and beyond the maternal morbidity and mortality associated with intended pregnancies. Some of these health outcomes include low birth weight, increased risk of preterm birth, and lower educational attainment (Dehlendorf et al., 2010; Hall et al., 2017). Other negative outcomes include relationship, mental, and financial stressors; reduced educational and career opportunities; and adverse outcomes for offspring (Abajobir et al., 2016; Goossens et al., 2016; Barton et al., 2017; Gariepy et al., 2017). These negative outcomes disproportionately impact people of color, people of low socioeconomic status, and adolescent/vulnerable populations (Dehlendorf et al., 2010; Francis et al., 2018; Geller et al., 2018). Additionally, 40% to 66% of global unintended pregnancies end in abortion, which is further associated with negative health outcomes (Finer and Zolna, 2016; Bearak et al., 2020). Finally, unintended pregnancy also correlates with negative outcomes in male partners, though studies on men and their experiences with unintended pregnancy are scarce (Kagesten et al., 2015; Kane et al., 2019).
In addition to unintended pregnancies, another often cited reason for the development of new contraceptive methods, especially male contraceptives, is the currently unsustainable rate of population growth and its effects on conservation and the environment (Rock, 1961; Short, 2009; Anderson, 2019; Page et al., 2022). However, while the global population is expected to grow, it is contradictory to specific instances of falling total fertility rates (TFR) in nearly all developed and even some developing countries. TFR refers to the average number of children a hypothetical cohort of women would have at the end of their reproductive period if they were subject during their whole lives to the fertility rates of a given period and if they were not subject to mortality, and it is expressed as children per woman (Pourreza et al., 2021). Studies have suggested that a TFR of 2.0 to 2.1 is required to maintain a stable population (Goodkind et al., 2018; Vollset et al., 2020). As of 2020, the world’s average TFR is 2.3, and the lowest and the highest TFRs in 2023 are represented by South Korea (0.78) and Niger (6.73), respectively (Susuman et al., 2016; Hwang, 2023). Many of the countries with very low TFR (e.g., Russia, Japan, and South Korea) are encouraging people to have more children through informational campaigns and policies to avoid potential population collapse. This may lead, either directly or indirectly, to the selective deprioritization of the development of new contraceptive methods for men or women in these countries or by those seeking to market in those countries. However, this ignores the importance of reproductive autonomy or for individuals to have the power to decide and control contraceptive use, pregnancy, and childbearing. The reproductive autonomy of men and women alike is currently limited because of a lack of contraceptive tools. For men, this contraceptive desert is particularly stark. From another standpoint, ignoring contraceptive development in favor of increasing TFR also ignores the need to give individuals and couples who desire one or more children the tools to plan and manage the timing and spacing of pregnancies. Since a male contraceptive prevents pregnancy in the female partner in a sexually active couple, effective male contraceptives will ultimately have an impact on men and women alike.
The need for male contraceptive options extends beyond the prevention of unintended pregnancy. Male participation in family planning is linked to positive social outcomes, including improved communication, shared decision-making, and improved gender equality across the relationship; it is also associated with positive health-related outcomes for female partners and offspring (Adelekan et al., 2014; Kraft et al., 2014; Ashfaq and Sadiq, 2015; Ruane-McAteer et al., 2020; Shand and Marcell, 2021). Expansion of the method mix to include novel male contraceptive options will contribute to enhanced family planning options and increase the positive outcomes realized by existing available methods (Dorman et al., 2018). In fact, willingness to use a novel male contraceptive is closely related to gender-equitable attitudes (Nguyen and Jacobsohn, 2023), suggesting that a positive feedback loop may occur wherein equitable gender attitudes increase male contraceptive acceptance and use, while male contraceptives themselves may positively influence gender equity and equitable attitudes at the same time. In addition, it stands to reason that contraception can act as a capture point for men in healthcare, wherein men seeking contraceptive services can undergo additional evaluations and improve their preventative care.
II. How Do Women and Men View a Potential Male Contraceptive?
As one of the most prescribed medications worldwide, combined oral contraceptive pills consist of two synthetic hormones: estrogen (e.g., ethinyl estradiol) and progestin (e.g., levonorgestrel) (Christin-Maitre, 2013; Sech and Mishell, 2015; United Nations Department of Economic and Social Affairs Population Division, 2019). The first birth control pill, Enovid, was approved for contraceptive use in the United States in 1960, and today ∼150 million women worldwide are taking the pill to prevent unintended pregnancy (Christin-Maitre, 2013; Sech and Mishell, 2015; United Nations Department of Economic and Social Affairs Population Division, 2019). Despite an efficacy of 99%, ∼850 million women are not using the pill but instead rely on other methods for contraception, e.g., intrauterine devices (hormonal and nonhormonal), implants, intravaginal rings, tubal ligation, spermicide, barriers (diaphragm, condoms, and sponge), etc., for various reasons, e.g., preference, convenience, efficacy, duration of use, availability, cost, and side effects. The fact that the unintended pregnancy rate remains high despite the many contraceptive methods that are currently available strongly suggests that there is an unmet need for contraception, which can be due to availability; affordability; or cultural, sociological, or psychologic restraints, to name a few reasons. One outstanding gap is that only two contraceptive methods are currently available for men (condoms and vasectomy), compared with more than 10 for women (pill, IUD, tubal ligation, diaphragm, condoms, sponge, ring, spermicide, implant, etc.). Consequently, this leads to women taking at least two-thirds of the contraceptive responsibility (Campo-Engelstein, 2012). This inequality is not due to men’s reluctance to use novel contraceptive methods but rather is caused by a lack of alternative, reversible methods being made available apart from vasectomy and condoms.
The literature has consistently reported meaningful hypothetical male and female interest in male contraceptive methods as well as realized interest and acceptability of methods being tested in a clinical setting (Heinemann et al., 2005; Cartwright et al., 2020; Nguyen et al., 2020, 2021b; Richard et al., 2022). Broadly, although there are differences among culture, geography, form of contraception, and other delineators, each finding reports that a substantial portion of men remains interested in a new and effective male contraceptive option (Glasier, 2010; Nguyen et al., 2021a). In published studies, the actual proportion of men willing to use a hypothetical contraceptive method varies from as low as 13.6% to as high as 83.0%, and in novel drug trials, the range is from 34.0% to 82.3%, indicating that exposure to and knowledge of male contraceptives may increase their acceptability (Male Contraceptive Initiative, 2021). Interestingly, despite being surveyed on delivery forms such as oral pills, shots, implants, transdermal gels, and vas-occlusive implants, no single form of contraception or frequency of administration is clearly favored by respondents in these surveys, providing further evidence that a variety of methods will be required to achieve maximal contraceptive utilization. It also indicates the need for further research into the nuanced differences of acceptability among various demographics or subgroups.
The partners of men are also broadly supportive of male contraceptive methods. A survey of almost 2,000 women noted that 87% of women thought a daily hormonal male contraceptive was a good idea and 98% of the total sample population said they would trust their partner with a daily oral pill (Glasier et al., 2000). Other studies demonstrate a strong interest from women in hypothetical or real-world contraceptives for men (Reynolds-Wright et al., 2021). It should be acknowledged, however, that the use of a male method does not require partner trust and that contraceptive use is not a zero-sum game. The introduction of a male contraceptive would likely result in at least some measure of combined contraceptive use where both partners in a relationship use their own contraceptive, resulting in better protection against unintended pregnancy. Similarly, many women may fully intend to continue their own contraceptive use regardless of their partner's use, although these settings and motivations are likely to be highly individualized and not always rooted in the prevention of pregnancy.
III. What Is the Market Size for Male Contraceptives?
While the broad interest indicates a significant market for novel male contraceptives, estimating an exact market size can be challenging as the usage of male contraception will depend on many factors, including the efficacy, safety, cost, availability, and cultural acceptability of the product. Market research activities that provide insights into the number of potential users for these methods and their preferences have been conducted. Conservative US market sizes for novel male contraceptives range from 12 million to >19 million men and a global market of >400 million men (Dorman and Bishai, 2012; Male Contraceptive Initiative, 2021). This market is driven by a wide range of motivations from potential users, which largely stems from the desire to prevent pregnancy and share responsibility for birth control. Men are also motivated by feelings of responsibility and dissatisfaction with current male and female methods. While men interested in new methods of male contraception largely see themselves taking a pill, either daily or just before intercourse, some of these motivations may be anchored by exposure to existing contraceptive methods, and a full suite of methods with other delivery modalities will likely be required to fully capture a contraceptive market.
Market research funded by The Bill and Melinda Gates Foundation and Male Contraceptive Initiative demonstrates significant interest in male contraceptive options and indicates potential for rapid uptake of new male contraceptive options across geographies. For example, 76% of men surveyed in Nigeria men reported expecting to take up a new contraceptive method within 1 year (The WHO/IBP Network, 2022). Data indicate other countries with high percentages of uptake within 1 year will be Bangladesh and Vietnam at 70%, Côte d'Ivoire at 62%, and Kenya at 52%. Interestingly, the United States had the lowest measured anticipated uptake at 39%; however, it is worth noting that these data were collected before Roe v Wade was overturned by the US Supreme Court in 2022 (Suppl. Table 1). A recent refielding of the research taking place after the Supreme Court decision saw the interest rise to 49% of men within 1 year of availability. Intention to use a male contraceptive at some point is similarly high, with >70% of men in all listed geographies stating an interest in ever using a potential male contraceptive method, and in some cases, e.g., Vietnam (98%), ever-use numbers approach complete saturation. This study also evaluated female partner interest in using a potential male contraceptive and found it to be >70% in all measured geographies, only marginally lower than among men (The WHO/IBP Network, 2022). Additionally, administration and frequency of use were shown to be the largest drivers of choice of novel male contraceptive methods. Interestingly, on-demand oral contraceptives, daily oral methods, and topical gels were of the highest interest to new users, as well as multipurpose prevention technologies that can simultaneously offer contraceptive and anti-infective benefits.
IV. Why the Long Delay with Male Contraceptives?
Male contraceptives have been in development by the academic, public, and private sectors in varying capacities since at least the early 1960s, yet there have been no new products come to market in that time (Heller et al., 1961). This disappointing reality results from a combination of factors, but one major challenge is a lack of support from the pharmaceutical industry, despite the obvious public health need and considerable public interest in these products. While involved until the mid-2000s, pharmaceutical companies have since abandoned contraceptive development programs altogether. Despite the lack of industrial support, hormonal male contraceptives have been in active development in multiple forms, including oral pill, injectable, and transdermal gel, which are comprised of combined synthetic forms of testosterone and progestin or progestogenic androgens that activate both androgen and progesterone receptors (Wang and Swerdloff, 2022). Other pharmacologic forms of male contraceptives are envisioned to use a nonhormonal approach, although these methods are comparatively early in development.
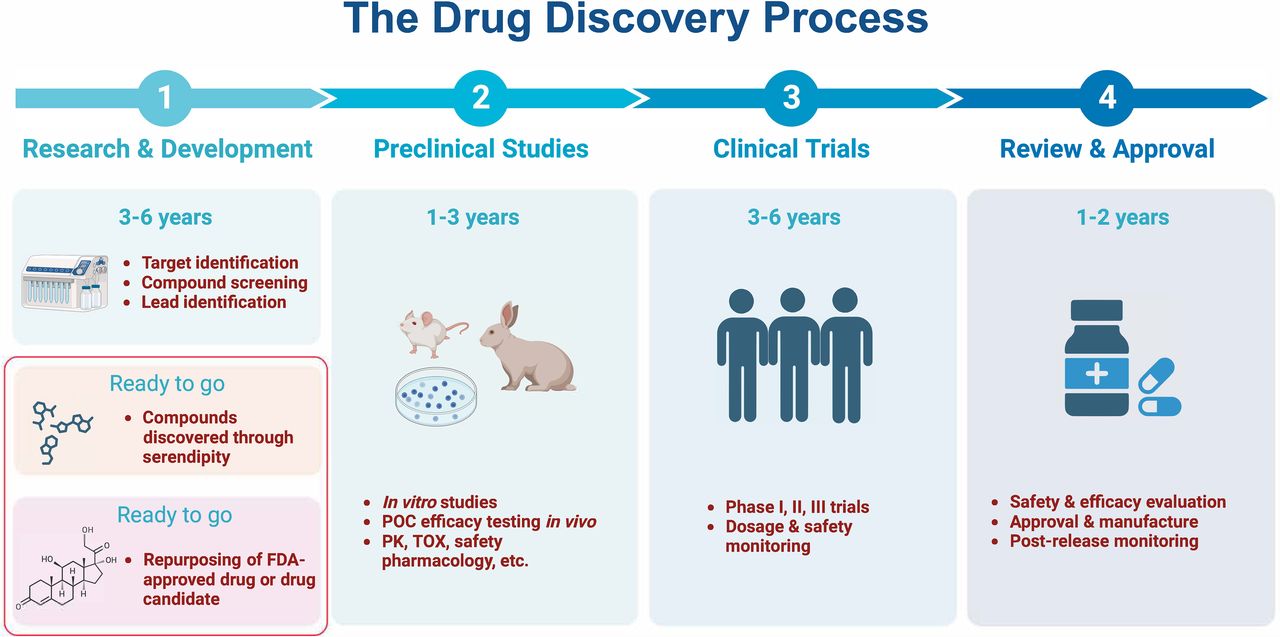
When considering the typical small molecule drug development pipeline, it often starts with drug target identification through biochemical and/or genetic screening (Fig. 1). These approaches can validate contraceptive targets or provide evidence that modulation of the target will result in infertility. However, the identification of a druggable target is typically the first step in a process that is many years away from a therapy being tested in humans. This is due to the existence of numerous so-called “valleys of death”: challenging stages of drug development where promising drug candidates often face significant financial and scientific obstacles before reaching the market, potentially leading to their abandonment. Even prior to the development of a drug candidate, it can be a risky process to identify compounds that interact with druggable targets. For example, it is possible that suitable hit compounds may not be identified to bind the target or the compounds identified may cause severe toxic effects, raising safety concerns. After a compound is identified to have effects in a laboratory animal model (often rodents) without discernable side effects, this compound still may not work on humans. For example, alkylated imino sugar n-butyldeoxynojirimycin, a Food and Drug Administration (FDA)-approved medication for Gaucher disease type 1, was first serendipitously reported to exert reversible contraceptive effects in mice (van der Spoel et al., 2002), but subsequent testing in humans did not demonstrate contraceptive effects (Amory et al., 2007). While animal models are often the most translatable and widely accessible approach to assess safety and efficacy of new drugs, studies in animals can be costly and time-consuming, further widening the valley of death for academic and startup entities in a field with no downstream industry support. On average, it takes 6 to 8 years for a drug candidate with excellent proof-of-concept efficacy testing results in both a rodent and a primate species to collect data required by the FDA for filing an Investigational New Drug application pursuant to first-in-human clinical trials (Fig. 1). Moreover, identification of a drug target or a lead compound represents just the very beginning of the lengthy drug development process. It is, therefore, incumbent on both researchers and media outlets to keep discoveries in context when a new druggable target is discovered or a compound is found to cause temporary infertility in translational animal models such as mice.

The timeline for the typical drug discovery process, which can be accelerated by including serendipity drug discovery and repurposing of existing drugs or drug candidates (framed).
V. Why Is Serendipity Observation Important in Drug Discovery?
In drug discovery, once a druggable target is identified, high-throughput screening of compound libraries can be employed to identify hit molecules that interact with the target. In contrast, serendipity drug discovery, although well known in the history of drug discovery, is far less common despite the fact that ∼20% of the pharmaceuticals in clinical use today are chemical derivatives of drugs discovered serendipitously (Ban, 2006). Male contraception is no stranger to serendipity discovery, as multiple putative male contraceptives have been isolated from natural sources (Kong et al., 1986). One example is gossypol, a polyphenol isolated from the seed, roots, and stem of the cotton plant (Gossypium). It is also present in cotton oil, and, in 1929, people who consumed cotton oil were serendipitously found infertile, and the compound causing male contraceptive effects was later determined to be gossypol (Yu and Chan, 1998). The subsequent clinical trials in China and Brazil showed that gossypol indeed could induce male infertility by causing spermatogenic arrest. However, its further development as a male contraceptive drug was suspended due to concerns over high rates of hypokalemia (0.75%) and poor reversibility, with 5% to 25% of the subjects becoming permanently infertile (Waites et al., 1998; Coutinho, 2002).
The latest example of serendipitous drug discovery comes from the Chinese herb T. wilfordii Hook F, commonly known as lei gong teng or thunder god vine. After some of the men who took this Chinese herbal medicine for an extended period (>3 months) displayed compromised fertility, physicians took note and were able to identify it as a cause of infertility (Qian, 1987; Matlin et al., 1993). Unfortunately, the subsequent research on the use of this herb or compounds isolated from this herb as male contraceptive agents found that either the crude herbal extracts or several of the most abundant compounds could indeed cause male infertility, but all were found to exert varying toxic effects (Chaudhury, 1993; Matlin et al., 1993; Ye et al., 1994; Ni et al., 2008). However, recently, a less abundant compound in this herb called triptonide was tested and found to be safe and effective in causing sperm deformation and male infertility in a reversible manner (Chang et al., 2021). Further testing of triptonide will be required to fully evaluate its potential as a male contraceptive, but history tells us that serendipity plays an important role in drug discovery and thus should be an integral part of the efforts in developing nonhormonal male contraceptives.
VI. Why Is Depleting Sperm or Spermatogenic Cells for Male Contraception Problematic?
Among the many reasons for the failure to develop a male pill, the vast difference in reproductive physiology between men and women may be a major contributor to the lack of observed progress. During reproductive ages, women undergo cyclic changes in hormonal levels each month, which are precisely controlled by the feedback system constituted by the hypothalamus-pituitary-ovary axis (Bliss et al., 2010; Henriet et al., 2012). By disrupting the cyclic patterns of female hormones, female hormonal contraceptives can effectively block folliculogenesis and thereby pregnancy. In contrast, men do not display monthly cyclic changes in their hormone levels, although androgen levels have been shown to display a diurnal rhythm, which is not associated with overall fertility (Faiman and Winter, 1971; Brambilla et al., 2009). However, taking advantage of the suppressive effects of elevated testosterone levels on the hypothalamus and pituitary, the prototype of the testosterone-only male birth control method was initially developed as an injection for male contraception in the 1990s (World Health Organization Task Force on Methods for the Regulation of Male Fertility, 1990, 1996). While suppression of sperm counts to azoospermia was achieved in nearly 100% of Asian men, 70% of non-Asian men achieved the same level. The ethnic variations remain unclear but are most likely due to differences in sensitivity of the hypothalamic-pituitary-testis axis and the metabolism of androgens (Ilani et al., 2011). Through the addition of progestin, a combined hormonal method for male contraception was found to be effective in reducing sperm counts to a contraceptive threshold, and the contraceptive efficacy was comparable to female hormonal methods (Wang and Swerdloff, 2022). Since then, clinical trials of oral, injectable, and transdermal hormonal male contraceptives using a range of active androgenic and progestogenic pharmaceutical ingredients have been ongoing with some challenges due to side effects, e.g., depression and mood swings in some men (Behre et al., 2016). While hormonal male contraceptives are likely to be among the first products to enter the market, more options for male contraception are still needed as some men may prefer the use of nonhormonal alternatives, as discussed earlier.
Since fertilization requires the union of only one sperm and one egg, it was initially believed that to achieve a contraceptive effect in men, it may be required to eliminate all sperm in the ejaculate. However, the only way to achieve this is to eliminate all mature sperm or eliminate sperm precursor cells, including spermatids, spermatocytes, or even spermatogonia. These notions are flawed for the following reasons: First, it is unnecessary to eliminate all sperm to achieve a contraceptive effect in men because when total sperm counts are reduced even to severe oligozoospermic levels (<1 million/mL), the pregnancy risk is ∼2% per year—highly comparable to effective female methods of contraception (World Health Organization Task Force on Methods for the Regulation of Male, 1996; Wang and Swerdloff, 2022). Second, both sperm and spermatogenesis have evolved to be resilient to disruptions to ensure the perpetuation of a species via sexual reproduction, and eliminating all sperm or their precursor cells is a very difficult proposition. It has been reported that sperm survive up to 24 to 48 hours after a man’s death (Golshan Iranpour and Rezazadeh Valojerdi, 2013). This resiliency is understandable given that oocytes are very limited in quantity, and, to ensure successful reproduction, the other gamete type, sperm, must therefore be produced in a much larger quantity and be able to survive insults from their microenvironments (reproductive tracts of both male and female) and macroenvironments (physiologic conditions of the host body). Third, spermatogenic cells tend to express multiple transcript and protein isoforms from the same genes (Zhang et al., 2017; Suzuki et al., 2019; Guo et al., 2022). In addition to the isoforms shared by somatic cell types, spermatogenic cells often express their own version of transcripts and proteins. If a compound targets a protein essential for spermatogenesis and this protein happens to have paralogs in somatic cell types, there is the potential likelihood that this compound could exert undesired off-target effects. Lastly, the high efficiency of sperm production in men renders the elimination of spermatogenic cells hard to achieve. Unlike folliculogenesis, spermatogenesis is a continuous process through which sperm are constantly produced. It has been estimated that ∼1,000 sperm are produced each second (Griswold, 2016). Female gametes, the oocytes, are ovulated in small numbers during each cycle and are located in an anatomically safer place relative to sperm, i.e., oviducts/Fallopian tubes. As the only human cell type with a primary function outside of the body in which it is produced, sperm, by contrast, must take a long journey, starting from the testis, then to the epididymis for maturation, through the prostate gland and urethra for ejaculation, followed by migration through the vagina and cervix to the uterine isthmus, and finally to the ampulla of the oviduct/Fallopian tube to fertilize an ovum. During these treacherous journeys, the vast majority of sperm are lost, with only a few successfully reaching the ovum. To compensate for the great loss, sperm must be produced in a larger quantity, which requires a much higher efficiency of spermatogenesis compared with folliculogenesis.
Gene knockout studies over the past several decades have identified hundreds of genes that are essential for spermatogenesis, sperm function, and male fertility. Many of these genes encode druggable targets and thus may be investigated as targets for developing male nonhormonal contraceptive drugs (Kent et al., 2020). However, as mentioned earlier, genes that play an essential role in mitotic male germ cells, i.e., spermatogonia, are often expressed as different isoforms of the same genes and tend to have paralogs in somatic cells (Eddy, 1998; Kleene, 2005). This may explain why the number of genes encoding druggable targets exclusively expressed in spermatogonia is relatively limited compared with those in spermatocytes and spermatids (Matzuk and Lamb, 2008; Kent et al., 2020). Many genes are exclusively expressed in spermatocytes and play an essential role in meiosis, a subset of which represent druggable targets (Matzuk and Lamb, 2008; Kent et al., 2020). Disruptions of these spermatocyte-specific genes, if causing severe meiotic defects, would likely lead to apoptosis due to the checkpoint mechanism (de Rooij and de Boer, 2003; Lei et al., 2023). However, if the defects are minor, the implicated spermatocytes may escape from the surveillance mechanism, progress through meiosis, and become haploid spermatids (Handel and Schimenti, 2010), which may increase the chance of fertilization and subsequent potential birth defects due to aneuploidy and other chromosomal defects in offspring (Fig. 2). Moreover, disruptions of the mitotic, meiotic, or early haploid phase of spermatogenesis will cause depletion of spermatogenic cells, triggering the hypothalamus-pituitary-testis axis and leading to elevated gonadotropin secretion, which may be of concern for some people in the context of long-term product use.

Comparison of drug development strategies that target various testicular and post-testicular cell types. HPT, hypothalamus-pituitary-testis; N/A, not applicable.
In contrast, disruptions of late spermiogenesis, the process through which round spermatids, the haploid male germ cells, differentiate into elongating and elongated spermatids without proliferation, rarely cause germ cell depletion despite the ongoing errors in the sperm assembly process (Yan, 2009; O’Donnell, 2015). Consequently, the resulting sperm generally display gross deformations and/or compromised motility, rendering them almost always incompetent for fertilization. Late spermiogenesis (from elongation onwards) appears to lack a checkpoint mechanism comparable to earlier steps of spermatogenesis, which also explains why a significant proportion of sperm (30%–40% in both mice and humans) are morphologically abnormal in the ejaculates of fertile males (Yan, 2009; Menkveld et al., 2011). Therefore, a drug that targets late spermiogenesis represents a high-priority approach for a novel male contraceptive because it will not cause depletion of male germ cells, thus maintaining testis size and even sperm counts without triggering the hypothalamus-pituitary-testis axis (Fig. 2).
Hundreds of genes have been identified to be uniquely expressed during spermiogenesis (Matzuk and Lamb, 2002, 2008). It is plausible to assume that drugs that target the resulting proteins would be far less likely to elicit somatic side effects, given that they are exclusively expressed in haploid male germ cells (Fig. 2). Based on this rationale, it has been proposed that targeting genes and gene products exclusively expressed during late sperm assembly represents a novel and high-priority idea for male nonhormonal contraceptive development (Yan, 2009). Of note, the approach of disabling sperm has been validated by two recent breakthroughs in male contraceptive development (Chang et al., 2021; Balbach et al., 2023), as discussed next.
VII. Novel Methods Currently in Development
Although a novel male contraceptive remains elusive, there are many academic and small-pharma programs intent on developing new methods for men, utilizing a wide range of active pharmaceutical ingredients, delivery methods, and mechanisms of action (Suppl. Table 2). For the purposes of this review, only male contraceptives with a demonstrated pharmacological mechanism are discussed in detail, although thermal and vas-occlusive methods of reversible male contraception are in development and rely on thermal dysregulation of spermatogenesis, and obstructive, dissolvable, or degradable implants, respectively (Lohiya et al., 2001; Soufir, 2017; Khourdaji et al., 2018; Long et al., 2021; Joubert et al., 2022).
To optimize the uptake of novel contraceptive methods for men, an array of hormonal contraceptive products with distinct product profiles are currently in development (Blithe, 2016). Daily-administered methods include oral pills (Attardi et al., 2006; Thirumalai et al., 2019; Wu et al., 2019; Yuen et al., 2020) and a transdermal gel that is rubbed on the shoulders (Anawalt et al., 2019). Longer-acting methods include an intramuscular injectable formulation with an onset time of some months as well as a subcutaneous implant with envisioned long-term efficacy (Nieschlag et al., 2013; Long et al., 2021). When tested clinically, these methods are generally well tolerated by users, and recent studies show high (>70%) user acceptability of daily oral hormonal pills (Nguyen et al., 2020, 2021b). As mentioned previously, while some clinical trials have reported adverse events and in one case the early termination of a study (Behre et al., 2016), more recent studies have reported no serious adverse events together with promising safety and efficacy. One specific challenge facing the development of hormonal contraceptives for men is a 2- to 3-month time to onset of a contraceptive effect following use initiation, similar to the time required for a vasectomy to be considered effective. A similar period is also expected for sperm counts to recover when discontinuing hormonal methods. This is also a challenge common to all drug-based methods that will impact early stages of spermatogenesis, as a full spermatogenic cycle takes 64 to 72 days in men (Heller and Clermont, 1964).
Nonhormonal methods of male contraception are also in development and may offer benefits over their hormonal counterparts through target specificity as well as the potential for more diverse product profiles. For example, while hormonal male contraception is limited to a mechanism of action that suppresses the earliest stages of sperm production, later-stage sperm development and other sperm functions can be targeted for contraceptive purposes, which can have a shorter time-to-action. Sperm maturation in the male reproductive tracts and sperm capacitation in the female reproductive tract are complex processes governed by a multitude of druggable targets. Focusing on unique targets with functions late in the life of sperm can lead to products with significantly lowered onset times, even to the point of an on-demand contraceptive. Additionally, since male contraceptive research and development largely exists in the discovery or early development stages, many programs are at a point where a delivery mechanism is yet to be identified and could significantly influence a product profile. While drug-based nonhormonal contraceptives have the chance for fewer side effects than their hormonal counterparts, only results from clinical safety studies will provide evidence of their true safety and specificity. However, methods that impact spermatogenesis will have a clear and easily quantified biomarker in sperm counts, whereas other mechanisms of action focused on sperm function may have less clear diagnostic outputs.
Much of the nonhormonal landscape consists of researchers at academic institutions, but two pharmaceutical companies, Eppin Pharma and YourChoice Therapeutics, are developing their small molecules, EP055 and YCT529, respectively, as daily oral contraceptives (Vitale, 2022). EP055 targets the epididymal-derived sperm surface protein EPPIN (epididymal protease inhibitor), which inhibits the protease prostate-specific antigen and binds semenogelin (SEMG1) (O’Rand et al., 2016). Binding of EP055 to the protein-protein interaction site between EPPIN and SEMG1 with EP055 results in a decrease in internal sperm pH and loss of intracellular calcium, ultimately leading to a loss of sperm motility (O’Rand and Widgren, 2012; O’Rand et al., 2018). Due to its impact on sperm function, rather than spermatogenesis, it is likely that the onset time for EP055 will be significantly shorter than that of hormonal or other spermatogenic-targeting methods. YCT529 on the other hand, targets the retinoic acid receptor alpha, preventing chromatin relaxation and gene expression in undifferentiated spermatogonia, causing developmental arrest (Noman et al., 2020). Blocking retinoic acid receptor alpha not only arrests spermatogenesis, but additionally impairs spermiogenesis.
As mentioned earlier, triptonide is a nonhormonal small molecule in development that was originally isolated from the natural plant source Trypterigium wilfordii. Recently, it demonstrated long-term contraceptive efficacy and initial safety in both mice and nonhuman primates (Chang et al., 2021). Oral intake of triptonide daily (0.8 mg/kg B.W.) can induce sperm deformation and severely compromised motility after 3 weeks in mice, but sperm count and testis size remain unchanged because germ cells were not depleted. Oral administration of triptonide (0.1 mg/kg B.W.) induces similar effects in nonhuman primates, except they also displayed slightly reduced sperm count and testis weight. After triptonide treatment is stopped, fertility is regained in 3 to 4 weeks in both mice and monkeys. Offspring fathered by fertility-recovered male mice and monkeys show normal growth and fertility. Early safety data on triptonide are also promising in both these species. Both short- and long-term treatments of triptonide cause no weight loss, no cancer development, and no pathologic changes in the vital organs of mice. In monkeys, no weight loss was observed, and blood panels showed normal liver, kidney, and immune functions even after triptonide treatment of ∼2.5 years. Triptonide’s mechanism of action appears to involve the binding of junction plakoglobin (also called gamma catenin), interfering with interactions between junction plakoglobin and SPEM1, which are required for the last several steps of sperm assembly. Triptonide represents a promising pathway toward a male contraceptive. However, further validation is required to clarify triptonide’s target and mechanism of action.
Another notable small molecule program in preclinical development includes antagonists of ADCY10, or soluble adenylyl cyclase (sAC). As a contraceptive target, sAC is unique as it functions to generate cyclic AMP in response to high concentrations of calcium ions and bicarbonate found in semen to initiate a process called capacitation, which occurs in the female reproductive tract and is essential for sperm to develop hyperactivated motility and ultimately reach the ampulla of the oviducts/Fallopian tube. Due to this mechanism, sAC could theoretically be developed as a male or female contraceptive. Moreover, as capacitation is a late-stage sperm function, if a quick pharmacokinetic distribution is assumed, sAC could be targeted to provide nearly on-demand contraception (Balbach et al., 2023). This does, however, mean that if delivered to a male user, inhibitors of sAC must be particularly long-lived, as ejaculated drug-containing semen will be quickly diluted in the female reproductive tract (Ferreira et al., 2022). The design of inhibitors with particularly long dissociation rates may facilitate inhibition of sperm motility long enough that sperm ejaculated from a male user are eliminated by the harsh vaginal environment, thereby granting a contraceptive effect. Recently, a company named Sacyl Pharmaceuticals was formed around this approach and is performing lead selection studies.
VIII. Perspectives
It is clear that development of male contraceptives is an important public health need and that efforts to develop them should increase substantially among funders, agencies, and private industry. This is especially pertinent in light of the fact that contraceptive drug development is a long and arduous road, even when the necessary funding is available. Based on the discussions here, many lessons have been learned from the past 50 years and new strategies to address field-wide challenges should be developed by taking the following into consideration: First, funding agencies should consider not only supporting research and development that utilizes canonical drug development strategies but also encourages drug discovery through serendipity observation (Fig. 1). Second, given that the testis has the largest transcriptome when compared with other organs and cell types, including cancer, many drugs or drug candidates that act on well-established targets in other organs and cancerous tissues may, in fact, have contraceptive effects and be good candidates for a male contraceptive. Reexamination of the “side effects” of existing therapies on the reproductive organs may help reveal effective, reversible male contraceptive agents among those already approved drugs or to-be-approved drug candidates, which may significantly expedite the drug discovery process for novel contraceptive options (Fig. 1). Third, no single method of male contraception will suit the needs of all users across their reproductive lifespans. The development of a full spectrum of products with a variety of characteristics will be required to optimize uptake. Finally, the users of male contraceptives are likely to be young, sexually active, and generally healthy men; thus, the development of a drug used by men with an indication of preventing pregnancy in a female partner is more challenging from a regulatory perspective than that for treating terminal illnesses or chronic disease. This is largely due to the particularly high safety and efficacy barriers that contraception presents when compared with other therapeutic areas, but it is also complicated by the fact that the FDA offers no specific guidance on the development of male contraceptives. Contraception also faces the challenge of pricing, where increasing cost can deter usage, even among those not financially vulnerable.
These combined developmental, regulatory, and financial risks appear to have made the pharmaceutical industry less motivated to develop male contraceptives, both hormonal and nonhormonal. This may partially explain why the industry has completely withdrawn from developing male contraceptives and largely withdrawn from the female contraceptive research and development sphere. Currently, nonprofit organizations, especially those backed by philanthropy and government, appear to be the major sources of funding for developing male contraceptives (Policy Cures Research Limited, 2023). Indeed, the Male Contraceptive Initiative is a philanthropic organization actively sponsoring research and development efforts specifically targeted toward reversible nonhormonal male contraceptives. However, the cost to get a drug to market can approach billions of dollars, and more support is necessary to buoy a scientific field where early development does not have the advantage of support from the pharmaceutical industry. Other philanthropic support for contraception is limited, with few organizations investing in development. This is primarily due to the fact that these organizations often favor women’s health, making support for male contraception an even smaller field within the small field of contraceptive research. However, the view that male contraceptives are for men alone and thus, unrelated to women’s health must be reconsidered as women bear the majority of risks and negative outcomes of unintended pregnancy. In that sense, developing effective male contraceptives is a women’s health issue and thus should be a priority topic for any funding agencies that support research that improves women’s health.
In summary, male contraceptive development has entered a new era where novel ideas have emerged and new promising drug candidates have been identified. Further development is underway, and the field is growing in scale and speed. To continue this trend, we must focus on specific considerations so that new ideas, new concepts, new methodologies, and new funding mechanisms can flourish. The goal of male contraceptive development should be to provide an abundance of options such that each individual user can find a method they agree with. Encouraging the development of a wide range of methods that rely on diverse mechanisms of action has the potential to generate products that real people use and potentially even enjoy. If we can do this, it is just a matter of time before pharmacies worldwide carry options that meet everyone’s needs.
Acknowledgments
The authors thank Christina Wang, Diana Blithe, George Gerton, and Ronald Swerdloff as well as Steve Kretschmer for their suggestions and comments during the preparation of this manuscript. Saayli Khambekar helped create the artwork in Figure 2. The authors apologize to colleagues whose work is relevant but not cited in this manuscript due to the scope and page limits.
Data Availability
The authors declare that all the data supporting the findings of this study are contained within the manuscript.
Authorship Contributions
Participated in research design: Nickels, Yan.
Performed data analysis: Nickels, Yan.
Wrote or contributed to the writing of the manuscript: Nickels, Yan.
Footnotes
- Received November 21, 2022.
- Revision received November 3, 2023.
- Accepted November 6, 2023.
This work was supported, in part, by grants from National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) [Grants HD071736, HD085506, HD098593, HD099924, and P30GM110767] (to W.Y.); National Institutes of Health/National Center for Advancing Translational Science UCLA CTSI [Grant UL1TR001881-01] (to W.Y.); and the Templeton Foundation [PID: 61174] (to W.Y.).
No author has an actual or perceived conflict of interest with the contents of this article.
↵
 This article has supplemental material available at pharmrev.aspetjournals.org.
This article has supplemental material available at pharmrev.aspetjournals.org.

Abbreviations
- AC
- soluble adenylyl cyclase
- FDA
- Food and Drug Administration
- TFR
- total fertility rate
- Copyright © 2023 by The Author(s)
This is an open access article distributed under the CC BY-NC Attribution 4.0 International license.
References
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- I. Male Contraceptive Development Is, After All, a Women’s Health Issue
- II. How Do Women and Men View a Potential Male Contraceptive?
- III. What Is the Market Size for Male Contraceptives?
- IV. Why the Long Delay with Male Contraceptives?
- V. Why Is Serendipity Observation Important in Drug Discovery?
- VI. Why Is Depleting Sperm or Spermatogenic Cells for Male Contraception Problematic?
- VII. Novel Methods Currently in Development
- VIII. Perspectives
- Acknowledgments
- Data Availability
- Authorship Contributions
- Footnotes
- Abbreviations
- References
- Figures & Data
- Info & Metrics
- eLetters
- PDF + SI