


Abstract
The human flavin-containing monooxygenase (form 3) (FMO3) participates in the oxygenation of nucleophilic heteroatom-containing drugs, xenobiotics, and endogenous materials. Currently, six forms of the FMO gene are known, but it is FMO3 that is the major form in adult human liver that is likely responsible for the majority of FMO-mediated metabolism. The substrate structural feature requirements for human FMO3 is beginning to become known to a greater extent and a few chemicals extensively metabolized by FMO3 have been reported. Expression of FMO3 is species- and tissue-specific, but unlike human cytochrome P450, mammalian FMO3 does not appear to be inducible. Interindividual variation in FMO3-dependent metabolism of drugs, chemicals, and endogenous material is therefore more likely due to genetic effects and not environmental ones. Examples of such interindividual variation come from the study of very rare mutations of the human FMO3 gene that have been associated with deficient N-oxygenation of dietary trimethylamine. Defective trimethylamine N-oxygenation causes trimethylaminuria or “fish-like odor syndrome”. Information on human FMO3 mutations from individuals suffering from the condition of trimethylaminuria has provided knowledge about the underlying molecular mechanism(s) for trimethylaminuria. A number of common variants of human FMO3 have been reported. Diversification of the FMO3 gene may have led to selective advantages and new functions. As more examples of human FMO3-mediated metabolism of drugs or new chemical entities are discovered in the future, it is possible that FMO3allelic variation may be shown to contribute to interindividual and interethnic variability of FMO-mediated metabolism. HumanFMO3 may be another example of an environmental gene that participates in a protective mechanism to help humans ward off potentially toxic exposure of chemicals.
The flavin-containing monooxygenases (FMOs1) (E.C.1.14.13.8) constitute a family of FAD-, NADPH-, and O2-dependent microsomal enzymes that catalyze the oxygenation of many nitrogen-, sulfur-, phosphorous-, selenium-, and other nucleophilic heteroatom-containing chemicals (Ziegler, 1980), drugs (Cashman, 1995), and agrichemicals (Hajjar and Hodgson, 1982). There are as many as six forms of mammalian FMO, and some can be present in multiple tissues of the same organism. Some of this information has been previously summarized (Cashman, 2002a). In humans, there is considerable interindividual and interethnic variability in the levels of FMO. In the past few years, a considerable increase in our understanding of the genetic variability of humanFMO has occurred and a summary of the current picture focusing on FMO3 will be presented.
Evidence for five functional forms of human FMO exist, each encoded by its own gene, that exhibit between 50 to 58% amino acid identity across species lines (Lawton et al., 1994). With the deposit of FMO6 into GenBank, an analysis of the protein encoded by this gene revealed that this protein shares 70% amino acid sequence identity with human FMO3, however, no function for this gene has been described. The description of multiple forms of FMO was advanced by elucidation of the primary sequences by amino acid (Ozols, 1990;Korsmeyer et al., 1998) and nucleotide analysis (Hines et al., 1994;Lawton et al., 1994; Phillips et al., 1995). As human FMOs were discovered, the common names assigned to enzymes were formalized and a nomenclature was adopted (Hines et al., 1994; Lawton et al., 1994). The nomenclature was developed on the basis of nucleotide sequence identity. If a human FMO gene has a sequence with ≥82% identity, it is grouped within a family, and the family is indicated by the first numeral of the designation (i.e., 1, 2, 3…). The order of naming followed the chronology of publication of the sequence for each member of the family (Dolphin et al., 1997b). The italicized prefix “FMO” is used to designate the gene or an allelic variant. Allelic variants have been observed for FMO that usually possess only single base changes. Other missense, nonsense, and deletion or truncation mutants of human FMO have been reported that can significantly affect enzyme function (Table1), and these will be discussed below in greater detail.
Genetic variation and amino acid substitutions of the human FMO31-a
Hepatic Human FMO
In the human, FMO3 is the prominent form in adult human liver, and other FMOs, if present, are expressed at very low levels as determined by mRNA analysis and confirmed by Northern blots (Lomri et al., 1992). The adult hepatic mRNA abundance is in orderFMO3≫FMO5≫FMO4 (Phillips et al., 1995). In human liver, FMO3 is quite abundant, approaching levels as much as 0.5% of total microsomal protein (Overby et al., 1997). Because FMO5 is an atypical FMO that does not show any of the typical activity against FMO substrates (Overby et al., 1995) and FMO4 activity is barely detectable (Dolphin et al., 1996b), FMO3 is the gene associated with the majority of FMO-mediated hepatic metabolism (Cashman, 2002a,b).
Human FMO3 Substrate Specificity
Human FMO3 possesses broad substrate specificity, accepting a wide variety of nucleophilic primary, secondary, and tertiary amines. In addition, nucleophilic sulfur-containing compounds are efficiently stereoselectively oxygenated by human FMO3 (Cashman, 1998; Cashman, 2002a). Human FMO3 apparently has some limitation on the size that tertiary amines are accepted for N-oxygenation (Lomri et al., 1993; Cashman, 2002a), but barring steric constraints, the prediction is that highly nucleophilic amines and sulfides are oxygenated by human FMO3 (Cashman, 2000).
Of note is the efficiency of human FMO3-mediatedN-oxygenation of primary amines to hydroxylamines and the subsequent N-oxygenation of hydroxylamines and eventual conversion to oximes. In mammals, efficient detoxication of potentially harmful hydroxylamines to oximes represents a way to terminate the pharmacological activity of primary amines (Lin and Cashman, 1997a,b;Cashman et al., 1999b). In contrast, in plants, FMO-like activity converts tryptamine to its hydroxylamine, and this metabolite possesses considerable growth-enhancing properties (Zhao et al., 2001). In contrast to the few number of FMO genes in humans, a large number of redundant FMO-like enzymes are present in plants, and this underscores its important role in plant cell differentiation.
Human FMO3 substrate activity appears to be dependent on chemical properties and shape (Cashman, 1995; Cashman, 2002a). Although it has been postulated that only one point of contact between substrate and enzyme is necessary for attack (Ziegler, 1993), stereoselectivity studies (Cashman, 1998) point to additional interactions in determining product formation. Generally, the Vmaxfor a wide variety of substrate is similar, andKm is variable but not precisely as a function of type or class of structure. The mechanistic details of FMO action have been summarized (Poulsen and Ziegler, 1979; Beaty and Ballou, 1981a; b; Jones and Ballou, 1986). Selective functional substrates for human FMO3 include trimethylamine (TMA) and (S)-nicotine. These amines are N-oxygenated on the tertiary amine atom (Cashman, 1995), and the interindividual variation will be discussed below.
Other nucleophilic heteroatom-containing compounds have been shown to be selectively oxygenated by human FMO3. For example, tamoxifen (Kupfer and Sehal, 1996), benzydamine (Ubeaud et al., 1999), xanomeline (Ring et al., 1996), N-deacetyl ketoconazole (Rodriguez et al., 1999), sulindac sulfide (Hamman et al., 2000) and itopride (Mushiroda et al., 2000) are substrates for human FMO3-mediated oxygenation. Methionine is also S-oxygenated by human FMO3 but only at high substrate concentrations (i.e., 10 mM) although FMO4S-oxygenates methionine at micromolar concentrations (Ripp et al., 1999).
The physiological role of FMO is unknown. However, FMO has been suggested to have evolved to detoxicate nucleophilic heteroatom-containing chemicals and xenobiotics found in foodstuffs by converting them to polar, readily excreted, water-soluble metabolites (Ziegler, 1990). FMOs have very broad substrate specificity and, barring steric limitations, accept most nucleophilic heteroatom-containing substrates for oxygenation (Cashman, 1995). It is notable that yeast FMO oxidizes biological thiols such as cysteine, cysteamine, and glutathione. Yeast FMO is active under conditions normally found in the cytoplasm but is inhibited as oxidized glutathione accumulates to give a redox potential similar to that found in the lumen of the endoplasmic reticulum. Yeast FMO may serve as a modulator of cell thiols and maintenance of thiol-disulfide redox potential (Suh and Robertus, 2002). It is likely that, as more species are investigated, the physiological role of FMO in cellular homeostasis will become clearer.
Extra Hepatic Human FMO
FMO1 is probably the most widely studied FMO largely because of its abundance in the liver of rodents and other animals. Human FMO1 functional activity is not detectable in adult human liver but is present during fetal development and is quite active in human fetal microsomes (Koukouritaki et al., 2002) or hepatocytes (Cashman, unpublished). In adults, FMO1 is not present in the liver to a detectable extent (Cashman et al., 1995; Phillips et al., 1995). Human FMO1 is present in human kidney and intestine and could in principle contribute to amine N-oxygenation but probably only at elevated substrate concentrations. Extra hepatic human FMO1 is capable of oxygenating certain substrates of limited size (Kim and Ziegler, 2000). Because FMO1 is present in the kidney and intestinal mucosa, it may play a significant role in metabolism of drugs or chemicals at these sites (Yeung et al., 2000). FMO1 is also present in the esophagus and nasal mucosa (Hines et al., 1994). It is possible that FMO1 serves in a “gatekeeper” function at the portals of entry of drugs or xenobiotics in the intestine or bronchial or central nervous system to metabolize materials and decrease the absorption of some chemicals.
Functional human FMO2 does not appear to be present in Caucasians (Dolphin et al., 1998). However, a functional FMO2 protein is present in as many as 26% of African Americans (Whetstine et al., 2000). Each of the FMO genes show a distinct pattern of development- and tissue-specific expression (Shehin-Johnson et al., 1995; Dolphin et al., 1996b). In addition to a prominent role of FMO3 in adult hepatic metabolism, FMO3 is also a major FMO in the brain. As in the case for interindividual variation noted for hepatic FMO3, human brain FMO3 variants may affect central nervous system drug metabolism. This may be especially important in the overall metabolism and pharmacokinetics of antipsychotic and other central nervous system (CNS) agents.
In the human brain, FMO3 is a prominent form, but human FMO4 and FMO5 are also present and, depending on the region of the brain, may represent major or minor isoforms (Bhamre et al., 1995). By a combination of immunological and reverse transcription-polymerase chain reaction methods, we have determined that in human substantia nigra, FMO3 is the prominent form, and FMO4 is present to a less extent (unpublished results). In the regions examined, FMO1, 2, 5, and 6 are not detectable in the adult human brain. Therefore, human FMO3 variants may affect CNS drug metabolism in the brain.
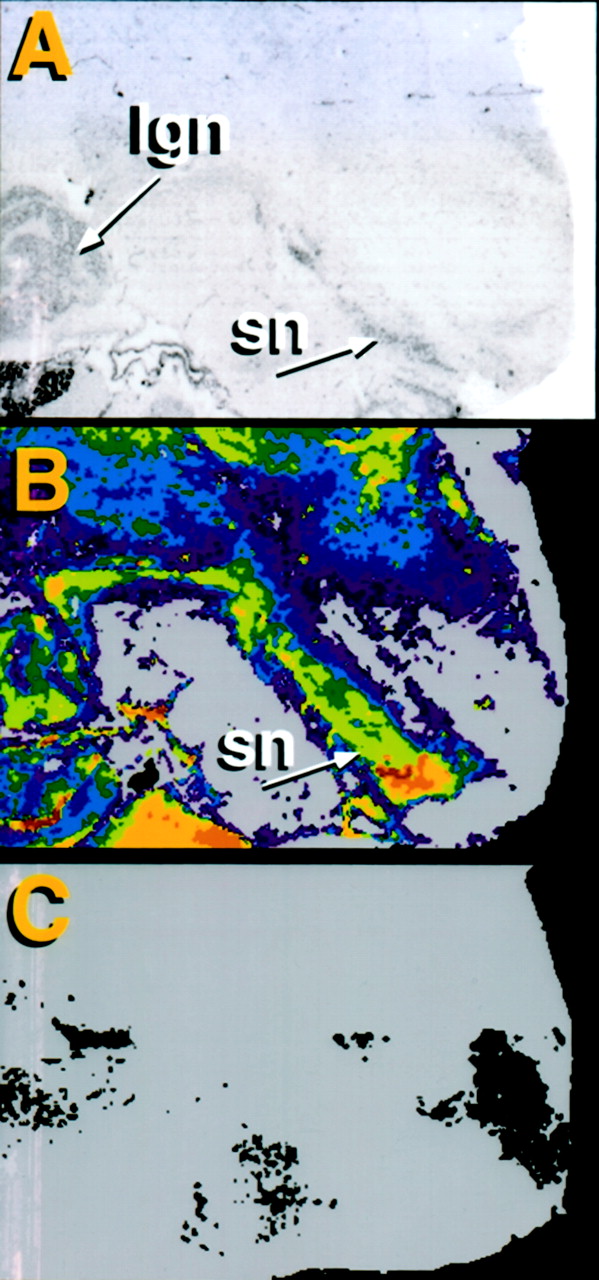
Figure 1 shows a human brain slice that contains the lateral geniculate nucleus (lgn) and the substantia nigra (sn) as marked in this negative immunostained silver slide. The middle panel (Fig. 1B) shows labeling of the tissue by a mono-specific antibody directed against human FMO3. There is a high density of labeling in the A10 region of the substantia nigra (shown by the red and yellow shading). Intensely immunoreactive cells are hot colors (red, yellow) and are representative of denser labeling than cool colors (green, blue, purple). The lower panel (Fig. 1C) shows an adjacent tissue section to 1B that was incubated in theabsence of primary antibody and represents nonspecific labeling of the hot secondary antibody. On the basis of the lack of labeling in Fig. 1C, immunolabeling in Fig. 1B is indicative of human FMO3. The immunolabeling work of Fig. 1 supports the fact that FMO3 is largely present in the substantia nigra of the human brain. Because of the notable genetic variability of human FMO3 observed thus far, human brain FMO3 may show considerable interindividual variation, and given the location of FMO3 in the substantia nigra and the proposed role of FMO in drug and chemical detoxication, it is possible that CNS drug metabolism may be critically dependent on FMO3.
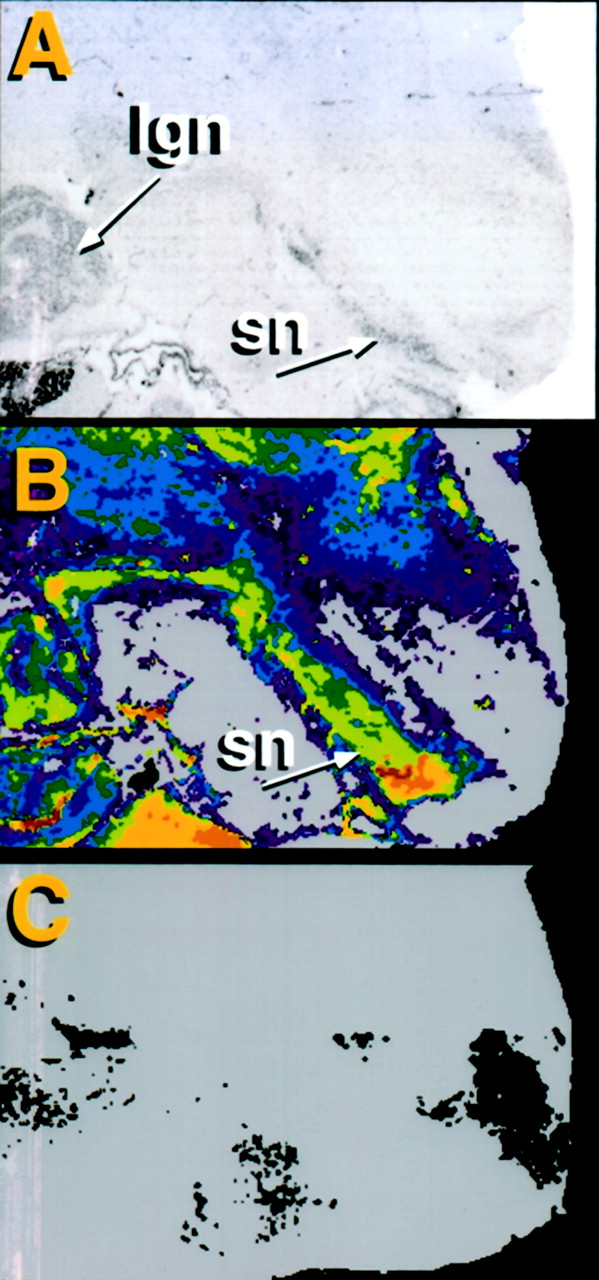
Immunolabeling of a normal human brain slice.
Panel A, a negative immunostained silver slide showing lgn and sn. Panel B, selective labeling of the A10 region of the substantia nigra by a mono-specific anti-human FMO3 antibody. Panel C, nonspecific labeling.
Interindividual Variability of Human FMO3 Functional Activity: In Vitro Considerations
Early studies with human liver microsomes showed considerable interindividual variability in functional human FMO3 activity. Now, we recognize that care needs to be taken to distinguish postmortem inactivation and FMO3 thermal degradation loss of enzyme function from variability due to genetic polymorphism-mediated FMO3 functional variation. Depending on the set of human liver microsomes studied, due to thermal inactivation, the range of FMO3 functional activity could be modest for some preparations of microsomes or completely lacking functional activity in other preparations despite the presence of significant FMO3 immunoreactivity.
Well characterized samples of human liver microsomes that were not thermally inactivated and showed that functional activity was highly correlated with immunoreactivity demonstrated a 6.6-fold variability in (S)-nicotine N-1′-oxygenation activity (Cashman et al., 1992) or a 2.7-fold variability of stereoselective (−)-4-bromophenyl-1,3-oxathiolane S-oxygenation activity (Cashman et al., 1993b) or a 2.4-fold variability of cimetidineS-oxygenation activity (Cashman et al., 1993a; Stevens et al., 1993). While a small amount of the variability observed may have been due to thermal degradation of FMO from mishandling of the tissue or improper storage of the liver or microsomes, most of the variability was likely due to genetic polymorphisms. In retrospect, the studies point out the importance of genotyping the individual samples in any set of human microsomes used.
A second study with another group of human liver microsomes illustrated the possible problems of human FMO3 postmortem inactivation. In this study, when human liver microsomal activity could be measured, a 400-fold difference in the N-oxygenation of 10-(N,N-dimethylaminopentyl)-2-(trifluoromethyl)phenothiazine was observed (Cashman et al., 1993b). However, three of ten microsome samples from this second set had no N-oxygenation activity despite in some cases possessing quite high FMO3 immunoreactivity. For this later set of human liver microsomes, it is likely that the FMO3 intersample functional variation was not dependent as much on genetic variability as it was on postmortem loss of FMO activity due to thermal denaturation. The studies show the importance of establishing a good correlation between FMO immunoreactivity and functional activity.
Human microsomal FMO3 levels have been reported to differ by 2- to 20-fold, but this depended on the age of the microsomal sample (Koukouritaki et al., 2002). Another report showed that as much as a 10-fold variation in human FMO3 content was observed (Overby et al., 1997), and this is in reasonable agreement with functional activity measurements (Stormer et al., 2000). In light of the variability in FMO3 functional activity as a consequence of genetic variation summarized herein and the confounding nature of FMO3 thermal inactivation, it is possible that use of carefully characterized human liver microsomes from fully genotyped tissue may diminish the ambiguity of doing in vitro evaluations. In addition, the use of well characterized hepatocytes or liver slices may also circumvent some of the variability associated with studying human FMO3-mediated oxygenations. For well characterized human liver microsomes, the interindividual variability in oxygenation of FMO-selective substrates is in reasonable agreement with the interindividual variability observed for in vivo pharmacokinetic parameters in humans (see below).
Interindividual Variability of Human FMO3 Functional Activity: In Vivo Considerations
The number of in vivo studies of selective FMO3 substrates is limited. Oxygenation of (S)-nicotine (Park et al., 1993), TMA (Treacy et al., 1998), cimetidine (Cashman et al., 1993a), clozapine (Sachse et al., 1999), and ranitidine (Kang et al., 2000) have been used to phenotype various populations for human FMO3 activity. All five materials have been shown to be relatively selective probes of human FMO3 activity in vitro. Each substrate has some advantages and disadvantages. (S)-Nicotine is selectively N-1′-oxygenated by human FMO3 to form exclusively the trans (S)-nicotineN-1′-oxide both in vitro and in vivo. Animal FMO1 forms a 50:50 mixture of cis and trans(S)-nicotine N-1′-oxide. Therefore, the stereochemistry of the product reveals whether FMO1 or FMO3N-oxygenates (S)-nicotine. That only thetrans (S)-nicotine N-1′-oxide diastereomer was formed in humans in vivo suggested that only FMO3N-1′-oxygenates (S)-nicotine (Park et al., 1993). Despite the usefulness of nicotine as a stereoselective in vitro probe of human FMO3, its use in vivo is somewhat limited due to the relatively high Km of (S)-nicotine for FMO3 and the fact thatN-1′-oxide is a minor metabolite. However, significant interindividual variability in the in vivo FMO3-mediated (S)-nicotine N-1′-oxygenation has been observed. Although only a small group of smokers were studied, the interindividual variation in the amount of urinary trans(S)-nicotine N-1′-oxide among 13 male smokers was significant and also dependent on the route of administration. The concentration of trans (S)-nicotineN-1′-oxide in the urine after free smoking varied 3.3-fold. Levels of urinary trans (S)-nicotineN-1′-oxide for the same smokers infused with (S)-nicotine-d2 varied 11.3-fold, and for those individuals administered (S)-nicotine via the dermal patch, N-1′-oxide formation varied 7.1-fold. It is notable that the fractional excretion of trans(S)-nicotine N-1′-oxide was significantly greater during free smoking compared with transdermal treatment (Park et al., 1993). This is in agreement with previous studies that showed considerable interindividual variability in metabolism and renal clearance of (S)-nicotine in humans (Benowitz et al., 1982).
TMA is an excellent substrate for FMO3 in vitro (Cashman et al., 1997;Lang et al., 1998) but because it arises from dietary choline and other sources, the TMA levels may vary in vivo. It is therefore important to not only determine TMA levels but also to establish in vivo TMAN-oxide/TMA ratios. TMAN-oxygenation is discussed in greater detail below. Cimetidine S-oxygenation is another selective substrate for human FMO3 presumably because of the nucleophilicity of the sulfur atom and because the imidazole nucleus serves to inhibit cytochrome P450-mediated oxidation (Cashman et al., 1993a). In humans, 75% of urinary cimetidine S-oxide formed is the (−)-isomer. The in vivo stereochemical result was in good agreement with that observed studying the S-oxygenation of cimetidine in vitro. The conclusion is that human FMO3 largely forms (−)-cimetidineS-oxide, and human FMO1 forms (+)-cimetidineS-oxide (Cashman et al., 1993a). The interindividual variability of cimetidine S-oxygenation in vivo was significant, although the variability was not as great as that observed for (S)-nicotine N-1′-oxygenation. Thus, the interindividual variation for the pharmacokinetic parameters of cimetidine S-oxygenation in seven healthy volunteers (i.e., area under the curve, t1/2 and CLR) was 2.6, 1.9, and 1.7, respectively. The explanation of the interindividual differences in cimetidineS-oxygenation may be due to the small population examined or possible presystemic intestinal FMO-mediated metabolism (Lu et al., 1998). Another explanation is that cimetidine S-oxygenation is under pharmacogenetic control.
Clozapine is a cyclic tertiary amine that is efficientlyN-oxygenated by human FMO3 (Tugnait et al., 1997). Clozapine and caffeine have been studied in vivo as probes of human FMO3 phenotype and genotype (Sachse et al., 1999). Whereas clozapine is an effective in vitro probe, three common polymorphisms of human FMO3 were not linked to either clozapine or caffeine metabolism. For clozapine, it is possible that the Km value is too high to serve as a useful in vivo marker (Sachse et al., 1999). The lack of correlation of caffeine with FMO3 (Rettie and Lang, 2000) brings up the issue as to whether caffeine is a useful probe for human FMO3. In view of the lack of a highly nucleophilic nitrogen atom and the lack of substrate activity, it is likely that caffeine metabolism is not dependent on human FMO3. Ranitidine N-oxygenation has found use in correlating phenotype with genotype in a Korean population (Park et al., 1999).
FMO Gene Organization
The human FMO5 gene is localized on chromosome 1q21.1 whereas the remaining members of the human FMO gene family,FMO1-FMO4 and FMO6 exist as a gene cluster at 1q23-q25 (McCombie et al., 1996; Dolphin et al., 1997b, Gelb et al., 1997). The human FMO3 gene spans a region of approximately 27 kilobases. Human FMO3 contains one noncoding and eight coding exons (Dolphin et al., 1997b), and the translation start codon is localized at the beginning of exon 2. For human FMO3, sequence analysis indicated that it has nine exons ranging in size from 80 to 705 base pairs. The general pattern of intron/exon organization for human FMO is similar to animal models, although this has not been extensively examined. For example, the intron/exon boundaries determined for human FMO3 (Treacy et al., 1998) relied on the gene structure of rabbit FMO2 (Wyatt et al., 1996). The intron/exon boundaries of monkey and chimp FMO3 are highly homologous (Cashman et al., 2001). The similarity in exon/intron organization for the FMO3 and other FMO genes may suggest that theFMO family members may have arisen from gene duplication and then further mutagenesis.
Diversification of the FMO gene presumably led to selective advantages and new function. This undoubtedly was geographical region-specific, and this may have contributed to the ethnic diversity of human FMO3 that is seen today. Because FMO has been suggested to play a role in detoxicating nucleophilic heteroatom-containing foodstuffs, it is possible that FMOplayed a role in certain niches of some populations to process some biological natural products and to protect that population. Further allelic variation of human FMO3 that alters the catalytic activity and or substrate specificity could render certain individuals or populations more or less susceptible to the effects of environmental xenobiotics. Human FMO3, for example, may be another example of an “environmental gene” that protects individuals from environmental chemical challenges and may represent an example of “animal plant warfare”. It is possible that evolutionarily conserved allelic variation of human FMO3 prevalent in certain geographical locations possessing certain plant toxins helped protect humans from plant toxin exposure (Gonzalez and Nebert, 1990). Because FMO3 metabolizes many materials to nontoxic substances that could otherwise inactivate P450 and because FMO and P450 are colocalized in the same region of the liver, it has been postulated that detoxication by FMO represents a chemoprotective strategy. A number of examples in the detoxication of sulfur- (Kedderis and Rickert, 1985; Decker et al., 1991; Cashman, 1995) and nitrogen-containing compounds (Cashman and Ziegler, 1986; Williams et al., 1989) have been put forth to support this hypothesis.
Biochemical Properties of FMO: Modulation and Regulation
In contrast to monooxygenases of the P450 family, there is little data to suggest that mammalian FMOs (other than FMO2) are inducible by small molecules. FMO2 levels appear to be regulated during development by pregnancy. Gestation increases FMO2 activity in rabbit (Shehin-Johnson et al., 1995). In the rat, some evidence has accumulated that hepatic FMO activity is decreased when animals are placed on a synthetic diet (Kaderlik et al., 1991). It is possible that hepatic FMO is maximally present and decreases to a de-induced level in the presence of a synthetic diet or other conditions (also see the section on “transient trimethylaminuria”, below). Hormones and dietary factors regulate FMO expression in a species- and tissue-dependent fashion. There is one report in the literature that rat FMO1 is induced by treatment of animals with 3-methyl cholanthrene (Chung et al., 1997), but this has not been independently confirmed. Expression of FMO is likely to be under the auspices of multiple mechanisms. That expression of FMO is tissue-specific comes from the observation that some tissues contain very high levels of FMO mRNA but very low levels of functional protein (Dolphin et al., 1998). For example, as discussed above, human FMO2 encodes a truncated nonfunctional protein and whereas white persons apparently do not express human FMO2, some individuals of African descent do possess full-length human FMO2. The expression of active human FMO2 will undoubtedly be highly dependent on the ethnicity of the population examined.
Because mammalian FMO is not induced by administration of low molecular weight chemicals or drugs, another way that FMO is regulated is via modulation by genetic polymorphisms. Genetic polymorphisms are defined as allelic variation occurring with a prevalence of at least 1%. Interindividual variation of enzymatic metabolic activity can result in significant population-wide differences in the oxygenation of drugs or xenobiotics. Polymorphisms of monooxygenase genes can exert a dramatic effect on drug metabolism. For example, CYP2D6-mediated debrisoquine 4-hydroxylation is ethnically linked: “poor metabolizers” make up about 5 to 10% of the population in the white population but only about 0.1% of the Asian population (Tucker et al., 1997). For those individuals that have the variant gene, the polymorphisms cause an exaggerated clinical response to the side effects of debrisoquine.
Common Polymorphisms of Human FMO3 Genes and Haplotype Analysis in Ethnic Groups
We analyzed the genotype of human FMO3 in individuals ascertained without regard to their health status. We examined the allelic frequencies and estimated haplotypes of non-Hispanic white persons, non-Hispanic African Americans, Hispanics, and Asians (Cashman et al., 2001). This is important fundamental information that needed to be established in a healthy population so that other study populations could be placed in the proper context. In addition, we studied the human FMO3 genotype for male and female white persons. The study was possible to rapidly accomplish because the genotyping procedure had been previously robustly worked out (Cashman et al., 2001). The samples were chosen randomly by a computer program for representative distribution of age and gender among the DNA bank. The wild-type human FMO3 gene, and the three prevalent polymorphisms (FMO3 158K, 257M, and 308G) were analyzed in 70 to 184 individuals per group (140–368 alleles). A relatively large number of alleles and polymorphisms could be examined because a chip-based mass spectrometric analytical method allowed high-throughput analysis. As shown in Table 2, there were significant differences among the ethnic groups examined for human FMO3 allelic frequencies. The linkage disequilibrium parameters D and D′ were used to compare the haplotype frequency differences and investigate the linkage disequilibrium. D was calculated for all pairs of sites in all four ethnic groups examined (Table 2). A test of overall linkage disequilibrium based on the number of observed and expected signs ofD showed a significant excess of disequilibria in which rare alleles were associated (Cashman et al., 2001). If the humanFMO3 257M or 308G allele contributes to decreasedN-oxygenation activity, it is possible that homozygous individuals possessing these alleles will detoxicate amines less efficiently and be at greater risk for exaggerated clinical response or adverse drug reactions compared with individuals with wild-type humanFMO3, but this needs to be experimentally verified.
Human FMO3 haplotype frequencies (sites 158–237–308)2-a
Table 2 lists the haplotype frequencies for three of the prominent polymorphisms described above (i.e., sites 158, 257, and 308). There are eight possible haplotypes for the three alleles examined. Two of the eight possible haplotypes (i.e., 158E-257M-308G and 158K-257M-308E) were not observed in the populations examined. It is interesting that certain haplotypes are significantly different for different populations. For example, Asians have a very high prevalence of the 158E-257M-308E haplotype but have a very low prevalence of the 158K-257V-308E haplotype. On the other hand, white persons, African Americans, and Hispanics appear to have a higher prevalence of the 158K-257V-308E haplotype. White persons, Asians, and Hispanics appear to have much higher prevalence of the 158K-257V-308G haplotype than do African Americans. In the populations examined, the 158K-257M-308G haplotype was only observed in Hispanics, and the 158E-257V-308G haplotype was quite rare appearing only in African Americans and Hispanics (Cashman et al., 2001). Currently, it is not known whether one particular haplotype is linked to abnormal amine metabolism (or a mild form of trimethylaminuria) or whether individuals with a particular haplotype are more susceptible to disease or adverse drug reactions. With the human FMO3 haplotype frequency differences in hand, linkage disequilibrium was investigated. A test of overall linkage disequilibrium showed a significant excess of cases of disequilibria in which rare alleles were associated (Cashman et al., 2001).
Evolutionary comparisons of FMO3 with sequences from a near species relative such as the chimpanzee, monkey, or baboon can illuminate features about human genetic variability. Such sequences can indicate those nucleotides that segregate in humans that might be ancestral. Certain sites may be conserved by chance or because the variation was not deleterious enough to be eliminated from the population via selection. However, the data accumulated thus far does not suggest any evidence for strong positive selection in theFMO3 genes (Cashman et al., 2001). For humanFMO3, it is possible that demographic forces rather than selection have played a role in creating haplotype differences. Of course, nonexon genetic variability may also play a role in determining the functional activity of human FMO3. For example, promoter or intron mutations may alter the transcription of human FMO3 and influence the functional activity.
Human FMO3 Polymorphism Analysis and Other Considerations
Because human FMO3 is apparently not induced by the administration of low molecular weight chemicals or drugs, population-wide differences in FMO3-dependent metabolism of drugs or xenobiotics are more likely due to genetic effects but not environmental ones. Interindividual variation of human FMO3 may contribute to the susceptibility of humans to exaggerated clinical responses or possible adverse reactions to chemicals or drugs. As discussed below, one extreme example of this is the inborn error of metabolism called trimethylaminuria. Ready identification of individuals presenting with elevated levels of urinary TMA has provided an efficient means of characterizing humanFMO3 genetic variation. To date, 24 variants have been observed and are listed in Table 1. Six of the 24 human FMO3variants (i.e., E158K, V257M, E308G, G180V, S147S, and F239F) have been observed to be associated with normal or slightly reduced TMAN-oxygenation activity (Cashman, 2002b). The first three variants are common polymorphisms, and the final three variants are somewhat rarer or code for synonymous substitutions. Of note is the possibility that two or more common polymorphisms when present in theFMO3 gene of the same individual contribute to a markedly more decreased human FMO3 activity. Another group of mutations listed in Table 1 were observed from analysis of DNA from individuals suffering severe or moderate trimethylaminuria (i.e., M66I, P153L, E305X, R492W, G148X, A52T, E314X, R387L, M82T, I199T, G475D, N61S, and M424I). Finally, the remaining variants either have not been conclusively associated with a severe trimethylaminuria phenotype or are synonymous changes that are unlikely to alter the phenotype. The possibility of idiopathic reactions related to rare or private humanFMO3 gene mutations comes from the observation that symptoms including hypertension, adverse tyramine reactions, depression, and other CNS effects are manifested in trimethylaminuria subjects (Treacy et al., 1998). A number of the CNS clinical outcome may be related to the symptomology. It is possible that individuals with decreased human FMO3 activity have the potential for altering the toxicity of drugs or chemicals and inducing adverse drug reactions. To date, no reports of variants unequivocally responsible for alteration of expression of human FMO3 have been reported. However, exhaustive analysis along these lines should be done. Care should be exercised about associating common genetic variations with decreased metabolism status because of the possibility that intron variability could be a prominent contributor to FMO3-mediated metabolism status. Some information about intron variability of human FMO3 is reported in Table3 and will be discussed below in greater detail.
Genotype frequencies of human FMO3 from african american and white persons: evaluation of exons and partial flanking intron regions3-a
An Example of a Human FMO3 Polymorphism Associated with Ethnicity
As discussed above, the approach we took to characterize the three prominent polymorphisms for human FMO3 assumed a sophisticated knowledge of the target gene and involved single nucleotide polymorphism analysis. After considerable additional work based on gene resequencing and mapping, we observed several FMO3 variants that were overlooked in the previous analysis. Thus, the variants described to date (Cashman et al., 2001) do not encompass the full extent of FMO3 variation present at the DNA-sequence level. It is likely that more FMO3 variants exist, and these will undoubtedly be population-specific. A systematic resequencing study of the entire FMO3 exonic regions and a substantial amount of the associated 5′- and 3′-flanking DNA showed numerous variable sites, many of which had not been previously reported. Of importance is to understand whether the FMO3 allele drifted to its current frequency by chance or is it selectively maintained? AreFMO3 variants linked? Are FMO3 variants associated with specific ethnic groups, and are population-specific distribution of alleles related to population-specific metabolism? The answer to these questions is currently not known, but recent studies examining DNA from white persons and African Americans have provided some insight.
As part of a larger effort to determine the frequency of variation in the FMO3 gene, a novel variant (GAT→CAT transition at codon 132) resulting in a change from aspartic acid to histidine was observed in 2 of 16 African Americans. Sequencing of DNA from 28 white persons did not show the presence of the D132H variant. cDNA expression of the variant and evaluation of prototypical FMO3 substrate activity showed that the D132H variant possessed significantly diminishedN-and S-oxygenation activity (B. Furnes, J. Zhang, A. Brooks, J. R. Cashman, and D. Schlenk, manuscript submitted for publication). In addition, a number of other exonic variants were observed that encoded silent mutations or substitutions, deletions, and additions within intronic regions (Table3). In a few cases, significant differences between the FMO3allelic frequencies of African Americans and white persons were observed (i.e., genomic DNA positions 1539, 21375, and 23516), but the biological significance of this variability is not known. However, most of these variations were observed randomly distributed among both white and African-American individuals and are not apparently linked to a specific population. It is unclear whether the FMO3 D132H variant is present in other ethnic groups, but it is possible that this variant may be relevant to drug and chemical metabolism in the African-American population.
Rare Human FMO3 Mutations
As described above, information regarding rare human FMO3 mutations has provided knowledge about an inborn error of metabolism called trimethylaminuria. Trimethylaminuria is an uncommon disease that is nonrandomly distributed in the population. However, in some parts of the world, especially in the tropics, there appears to be an elevated incidence of trimethylaminuria (Al-Waiz et al., 1987; Hadidi et al., 1995; Dolphin et al., 1997a; Mitchell et al., 1997; Thithapandha, 1997;Treacy et al., 1998). Individuals with trimethylaminuria possess a decreased ability to oxygenate diet-derived TMA. Under normal conditions TMA is N-oxygenated ≥95% to the odorless metabolite TMA N-oxide. Individuals unable toN-oxygenate TMA excrete large quantities of TMA in their urine, sweat, and breath and suffer from what has been called “fish-like odor syndrome” because of the fish-like odor (reviewed in Mitchell and Smith, 2001). For severely affected individuals suffering from trimethylaminuria as much as 90% of dietary TMA can go unmetabolized. It has been established that human FMO3 is largely responsible for TMA N-oxygenation and that defectiveFMO3 genes are responsible for trimethylaminuria and segregate with the disorder. The first studies focused on populations of British and Australian origin. A phenotype-genotype correlation emerged from the work that indicated many of the most severe trimethylaminuria cases could be explained by P153L, M66I, or E305X human FMO3 mutations (Dolphin et al., 1996a, 1997a;Treacy et al., 1998). cDNA-expression of these variants showed that they possessed minimal or no TMA N-oxygenation activity in vitro (Cashman et al., 1997; Dolphin et al., 1997). In some cases, homozygotes with the P153L or E305X genotype had urinary TMAN-oxide/TMA ratios of 10:90 or almost exactly opposite what is observed for normal urinary TMA N-oxide/TMA ratios. As other populations have begun to be examined for FMO3mutations associated with trimethylaminuria, several observations have come forward: 1) although quite rare, some of the human FMO3gene mutations have been jointly observed in different populations suffering from trimethylaminuria, and 2) as more populations are examined, additional very rare (or private) disease-causing mutations have been found. For example, as additional people from North America have been studied, some FMO3 gene mutations common to the British and Australian cohorts were observed, but new mutations (i.e., A52T, E314X, R387L) were also reported (Akerman et al., 1999). Today, a growing list of rare FMO3 gene mutations has been reported, and some are likely to be population-specific (see Table 1 for a summary).
Human FMO3 Variants Associated with Transient Trimethylaminuria
Sometimes young children or even adults have been reported to suffer from “transient” trimethylaminuria. In the case of young children (i.e., a 2-month or a 4-year old) (Mayatepek and Kohlmueller, 1998) the explanation could be that the child did not express detectable amounts of FMO3. Although highly variable, before birth, FMO3 is not expressed (Koukouritaki et al., 2002). After 1 to 2 years of age, most individuals express significant levels of FMO3. Intermediate levels of FMO3 are expressed until age 11 and then mature levels of FMO3 are observed from ages 11 to 18. It is possible that the transient trimethylaminuria observed in young children could resolve itself with age as the individual matures and once the full expression of FMO3 is realized (Koukouritaki et al., 2002).
Another example of transient trimethylaminuria has been observed for some individuals that possess the common variant allele (E158K; E308G). Some, although not all people possessing this variant have decreased TMA N-oxygenation after oral TMA challenge (Zschocke et al., 1999) when they are compound heterozygotic or homozygotic for E158K; E308G. The variability in the degree of trimethylaminuria for this relatively common allele (see Table 2) may lie with the requirement of an additional cis variant working in concert to decrease FMO3 activity. In addition, for these individuals, the trimethylaminuria condition may be exacerbated under certain dietary conditions (i.e., elevated TMA or elevated dietary precursors such as choline) or elevated diets of brassica vegetables (Fenwick et al., 1983) (that inhibits human FMO3) (Cashman et al., 1999a). Another example of transient trimethylaminuria for some women occurs during menstruation (Zhang et al., 1996). Yet another possible example of transient trimethylaminuria can occur in the case of individuals experiencing copper deficiency (Blumenthal et al., 1980). The reason why some adults and not others develop transient trimethylaminuria is unknown but may be explained in the future by additional biochemical and genetic studies.
The literature is replete with examples of adverse interactions with drugs and/or chemicals mediated by P450. One such example is the induction of CYP2E1 by ethanol or other related alcohols and ketones that metabolize disulfiram (Antabuse) to toxic species (Guengerich et al., 1991). For human, FMO evidence for such clear-cut adverse drug interactions have not been reported, but some examples of adverse clinical problems have emerged. For example, individuals with trimethylaminuria also suffer from additional metabolic and psychosocial abnormalities including low self-esteem, anxiety, clinical depression, and addiction to drugs (Todd, 1979). Many of these clinical manifestations could arise, at least in part, from abnormal endogenous or xenobiotic metabolism. For example, in the Australian trimethylaminuria cohort discussed above (Treacy et al., 1998), several individuals also manifested hypertension and adverse reactions from tyramine, other amines, and sulfur-containing medications. FMO metabolism of biogenic amines could contribute to some of the neurochemical effects observed in individuals with trimethylaminuria, and further studies are required to understand this more fully. One report showed that a trimethylaminuria patient produced seizures and other behavioral disturbances after subjected to choline loading (McConnell et al., 1997). Dietary choline is a major precursor source of TMA. Certain CNS drugs that are normally efficiently cleared could produce exaggerated responses for individuals with common polymorphic variants of FMO3 (Adali et al., 1998). For example, the metabolic detoxication of amphetamine and methamphetamine by human FMO3 may be under pharmacogenetic control (Cashman et al., 1999b). Anecdotal reports have suggested that tricyclic antidepressants give exaggerated side reactions for individuals suffering from mild or severe trimethylaminuria.
Conclusions
Recent studies of human FMO3 genetic variation have shown that a number of novel alleles encode rare mutations that abrogate or significantly reduce FMO3-mediated chemical metabolism. The discovery of these mutations has provided information about the underlying molecular mechanism(s) for trimethylaminuria. In addition to rare mutations, more common genetic polymorphisms have been revealed using modern genotyping methods. Although it is entirely likely that the number of human FMO3 variants observed will increase in the future, the present data suggests that common polymorphisms at variable sites 158, 257, and 308 shows significant heterogeneity in the relative frequencies of single and multiple site alleles, haplotypes, and genotypes. A population-selective FMO3 variant (D132H) with decreased activity may be relevant to drug and chemical metabolism status in African Americans. The variability of the common polymorphisms observed for human FMO3 as a function of different populations may portend population differences in the susceptibility of humans to abnormal metabolism or adverse drug reactions for chemicals or drugs metabolized by human FMO3. The observation that human FMO3 is a prominent FMO in the brain suggests that variants of brain FMO3 may impact the disposition of CNS agents or endogenous materials that are metabolized by FMO3 in the course of their detoxication, and this may contribute to determining an individual's metabolism status and susceptibility to adverse CNS effects.
Acknowledgments
We acknowledge the many collaborators and coworkers in our laboratory and in the laboratories of collaborating scientists that have been valuable contributions to the work discussed herein. We thank Drs. James Leushner and Andreas Braun of Sequenom Inc. (San Diego, CA) and Professor Ron Hines of Wisconsin College of Medicine (Milwaukee, WI) for stimulating discussions. We acknowledge the collaboration with Professor Daniel Schlenk and Bjarte Furnes of the University of California (Riverside, CA) on FMO3 D132H. We thank Deborah Mash and Dr. Sari Izenwasser of the University of Miami, National Institutes of Health Brain Bank (Miami, FL) for Fig. 1.
Note Added in Proof.
Recently, Hines et al. (2002) noted an explanation for the lack of functional activity of FMO6 due to alternative processing that encodes a non-functional FMO6 transcript.
Footnotes
- Received May 15, 2002.
- Accepted July 15, 2002.
- The American Society for Pharmacology and Experimental Therapeutics
References
 John R. Cashman obtained the bachelor degrees in chemistry and biology at the College of Creative Studies, University of California, Santa Barbara in 1977. He did undergraduate research in the lab of Professors Thomas Bruice and Paula Yurkanis Bruice on the bioorganic chemistry of isoalloxazines and flavins. He received his masters and doctorate degrees in Medicinal Chemistry from the University of Kansas, Lawrence, Kansas in 1982. His doctoral research involved studies of the chemical, enzymatic, and in vivo oxygenation of the thiocarbonyl functionality of thiobenzamides under the direction of Professor Robert Hanzlik.
John R. Cashman obtained the bachelor degrees in chemistry and biology at the College of Creative Studies, University of California, Santa Barbara in 1977. He did undergraduate research in the lab of Professors Thomas Bruice and Paula Yurkanis Bruice on the bioorganic chemistry of isoalloxazines and flavins. He received his masters and doctorate degrees in Medicinal Chemistry from the University of Kansas, Lawrence, Kansas in 1982. His doctoral research involved studies of the chemical, enzymatic, and in vivo oxygenation of the thiocarbonyl functionality of thiobenzamides under the direction of Professor Robert Hanzlik.
He completed his postdoctoral research in 1984 in the Department of Chemistry at Harvard University in Cambridge, Massachusetts with Professor E. J. Corey. His work involved the synthesis of arachidonic acid derivatives, studies of the mechanism of 5- and 15-lipoxygenase, and the leukotriene receptor. In 1984 he was appointed Assistant Professor of Chemistry and Pharmaceutical Chemistry at the University of California, San Francisco. His work involved the study of the molecular aspects of the human flavin-containing monooxygenase, arachidonic acid biochemistry, and biological and toxicological chemistry. Beginning in 1994, he was Senior Scientist at the Seattle Biomedical Research Institute and prior to that he was Associate Director for the IGEN Research Institute in Seattle, Washington. In 1997, he founded the Human BioMolecular Research Institute, a non-profit research institute dedicated to performing fundamental and applied research to address important human diseases of the central nervous system. He is consulted by biotechnology, pharmaceutical industry, and government in various areas of human drug development, drug safety evaluation, medical chemistry, pharmacogenetics, and biochemical toxicology. Dr. Cashman is on the Board of Directors of three life science companies.
 Jun Zhangreceived the B.S. degree in Biochemistry from Nanjing University, China, and the Ph.D. degree from State University of New York at Buffalo. She completed her postdoctoral research with Dr. Marie Hardwick at the Johns Hopkins University, studying Sindbis virus induced neuronal apoptosis. She joined Human BioMolecular Research Institute in 1999 establishing her research interests in studies of FMO enzymes and their potential neuronal protective function in brain.
Jun Zhangreceived the B.S. degree in Biochemistry from Nanjing University, China, and the Ph.D. degree from State University of New York at Buffalo. She completed her postdoctoral research with Dr. Marie Hardwick at the Johns Hopkins University, studying Sindbis virus induced neuronal apoptosis. She joined Human BioMolecular Research Institute in 1999 establishing her research interests in studies of FMO enzymes and their potential neuronal protective function in brain.
Footnotes
-
The financial support of the National Institutes of Health (DK59618) and the California Tobacco Related Disease Research Program (9RT-0196) is gratefully acknowledged.
- Abbreviations used are::
- FMO
- flavin-containing monooxygenases
- TMA
- trimethylamine
- CNS
- central nervous system
- lgn
- lateral geniculate nucleus
- sn
- substantia nigra
- P450
- cytochrome P450
- The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
Jump to section
- Article
- Abstract
- Hepatic Human FMO
- Human FMO3 Substrate Specificity
- Extra Hepatic Human FMO
- Interindividual Variability of Human FMO3 Functional Activity: In Vitro Considerations
- Interindividual Variability of Human FMO3 Functional Activity: In Vivo Considerations
- FMO Gene Organization
- Biochemical Properties of FMO: Modulation and Regulation
- Common Polymorphisms of Human FMO3 Genes and Haplotype Analysis in Ethnic Groups
- Human FMO3 Polymorphism Analysis and Other Considerations
- An Example of a Human FMO3 Polymorphism Associated with Ethnicity
- Rare Human FMO3 Mutations
- Human FMO3 Variants Associated with Transient Trimethylaminuria
- Conclusions
- Acknowledgments
- Note Added in Proof.
- Footnotes
- References
- Footnotes
- Figures & Data
- Info & Metrics
- eLetters