Article Text

Abstract
Background—Diagnosis of drug induced liver injury is usually based on a temporal relation between drug intake and clinical picture as well as on the exclusion of alternative causes. More precise diagnosis has been attempted by using in vitro specific T cell reactivity to drugs but the test has never reached general acceptability because of frequent negative results which could be explained, in part, by prostaglandin producing suppressor cells (PPSC).
Aim—To analyse the diagnostic value of a modified test where lymphocyte responses to drugs are detected in the presence of a prostaglandin inhibitor.
Patients—Ninety five patients with a clinical diagnosis of drug induced liver injury, 106 healthy controls, 35 individuals with recent exposure to the same drugs without adverse effects, and 15 patients with liver disease unrelated to drugs.
Methods—Peripheral blood mononuclear cells (PBMC) were cultured in the presence of drugs alone and in the presence of drugs and a prostaglandin inhibitor. Responses were assessed by3H-thymidine incorporation in lymphocytes. Results were expressed as counts per minute and as stimulation indexes (SI).
Results—When PBMC were stimulated with drugs alone, lymphocyte sensitisation to drugs (SI>2) was detected in 26% of the cases. This was noticeably increased (56%) when a prostaglandin inhibitor was added to the cultures. No reactivity was found in controls. In patients with possible sensitivity to several drugs, lymphocyte reactivity was detected to only one drug. The severity of the lesions, as assessed by aminotransferase concentrations and disease duration, was lower in patients with evidence of PPSC.
Conclusions—This new approach is useful for the diagnosis of drug induced liver injury, particularly in patients exposed to more than one drug; furthermore, the presence of putative PPSC is associated with less severe forms of drug induced hepatitis.
- drug induced hepatitis
- drug hypersensitivity
- specific T cells
- prostaglandin E2
- suppressor cells
- diagnostic tests
Statistics from Altmetric.com
- drug induced hepatitis
- drug hypersensitivity
- specific T cells
- prostaglandin E2
- suppressor cells
- diagnostic tests
Drug induced liver injury can occur as a result of dose dependent, intrinsic drug toxicity or by dose independent idiosyncratic mechanisms.1 Diagnosis of drug induced liver injury in the rare cases of dose dependent reactions is straightforward, whereas diagnosis of the more common dose independent adverse reactions relies on clinical criteria that are sometimes difficult to apply, particularly in patients exposed to more than one drug.2 ,3 Two different dose independent mechanisms may be involved in drug induced liver injury: allergic hypersensitivity, and metabolic idiosyncrasy associated with the accumulation of reactive metabolites. These can damage hepatic structures by direct mechanisms4 ,5 or can covalently bind to macromolecules (membrane or plasma proteins) and form an antigen, which in turn, elicits a hypersensitivity reaction.4-6 It has been suggested that in most cases of drug induced liver injury, even when metabolic idiosyncrasy is the initiating feature, immunological hypersensitivity can be involved as an effector mechanism.4 ,7
The most convincing evidence in favour of an allergic basis for the drug induced liver disorder is the demonstration of specific antibodies8 or sensitised T cells to the drug or its metabolites.9-13 Unfortunately, immunological tests are rarely performed in cases of suspected drug induced liver injury and in many published studies they are reported as negative.14 ,15 This could be a consequence of inadequate antigenic presentation of the drug or, alternatively, could be due to the presence of putative suppressor factors in the in vitro culture systems. We have presented evidence previously that several modifications to the test—namely, the addition of a prostaglandin inhibitor to the culture system16 ,17 and the use of ex vivo prepared drug antigens or metabolites instead of the parental drug,9 ,18 may improve detection of lymphocyte sensitisation to drugs in cases of drug induced hepatitis.
The list of drugs involved in liver injury continues to increase although it is usually accepted that no significant improvement in the accuracy of the diagnosis has occurred.3 ,19 In view of the new methods for studying in vitro sensitisation to drugs,16 ,18 it is important to assess the diagnostic value of such modified immunological tests in a large series of patients. In this study we present results of the in vitro lymphocyte reactivity to drugs in the presence of a prostaglandin inhibitor, tested in a series of 95 patients with a clinical diagnosis of drug induced liver injury, in order to clarify the diagnostic impact of this approach.
Methods
PATIENTS AND CONTROLS
Ninety five patients with a final clinical diagnosis of drug induced liver injury were investigated (table 1). They were consecutively referred to our unit for clinical opinion and immunological studies, between 1985 and 1996. Forty two of these patients were included in the initial study describing prostaglandin producing suppressor cells (PPSC) in drug induced hepatitis.17 Table 2 shows the clinical manifestations and alterations in liver tests observed in the patients studied. Jaundice was present in 69 (73%) patients and extrahepatic manifestations such as fever, rash, and eosinophilia were observed in 37, 28, and 33 patients respectively. The clinicolaboratory pattern observed in these patients was classified as cholestatic in 37, hepatocellular in 39, and mixed in 19, according to criteria by Danan.20 The diagnosis of drug induced liver injury was based on the establishment of a consistent temporal relation between drug intake and the onset of clinical symptoms and on the exclusion of alternative causes of liver injury—viral hepatitis, alcoholic liver disease, biliary tree obstruction, and pre-existing liver disease by standard criteria.2 Procedures used to rule out alternative causes included abdominal ecography in 88 (93%) patients, liver biopsy in 48 (51%), and endoscopic retrograde cholangiopancreatography in 20 (21%). Five patients were subsequently and inadvertently reexposed to the suspected drugs. The clinical symptoms reappeared in all of these patients. A diabetic, 22 year old man was accidentally reexposed three times to cotrimoxazole, with subsequent increases in liver enzyme concentrations.
Clinical characteristics of the patients studied
Clinical manifestations and alterations in liver function tests observed in patients with drug induced liver injury
Three types of controls—healthy controls (n=106), individuals with recent exposure to the same drugs but without adverse effects (n=35), and patients with liver diseases unrelated to drugs (n=15), were also studied (table 3).
Characteristics of the controls studied
PREPARATION OF DRUG SOLUTIONS
The drugs selected for study in each case were those with a significant probability of being involved in the liver lesion on the basis of the usual clinical criteria, with emphasis on the temporal relation between drug intake and adverse effect. Table 4 lists drugs tested in control subjects who had taken the drugs without developing adverse effects.
Drugs tested in controls with recent exposure to the suspected drugs without adverse effects
Drugs were dissolved in RPMI medium (Gibco) and left in a magnetic shaker for six hours. Drugs insoluble in aqueous medium were dissolved in 95% ethyl alcohol and diluted in RPMI medium, with a final concentration of alcohol below 0.002% which is known to be non-toxic to the cultures.21 Drug solutions were then ultrasonicated at 50 Hz for one minute and passed through a 0.22 μm millipore filter. Five dilutions of the drugs in RPMI were prepared, so that the median concentration corresponded to the mean plasma concentration observed in humans after the ingestion of a therapeutic dose of the drug; two concentrations above and two below were also used.
LYMPHOCYTE PROLIFERATION IN DRUG SOLUTIONS
Lymphocyte proliferation studies were performed as described previously.22 Briefly, peripheral blood mononuclear cells (PBMC) were isolated from heparinised venous blood, washed three times in phosphate buffered saline (PBS), and resuspended at a concentration of 1×106/ml in RPMI 1640 medium (Gibco) enriched with 15% inactivated fetal calf serum (FCS), 2 mM l-glutamine (Gibco), and 2% penicillin (100 U/ml)/streptomycin (100 μg/ml). In patients 57–95, 10% human AB serum (Sigma) was used instead of FCS, and penicillin/streptomycin was substituted with 20 μg/ml gentamicin (Sigma). PBMC (100 μl) were distributed to each well of a 96 well microtitre plate (Costar) and 20 μl of each drug concentration was added to the wells. Experiments were done in triplicate. Cells were cultured for six days at 37°C in a humidified, 5% CO2enriched atmosphere; 12 hours before the end of the cultures 1 μCi3H-thymidine (specific activity 23 Ci/mmol, Radiochemical Centre, Amersham, UK) was added to the cultures. Cells were harvested on filter discs and counted in a β-counter. Results were expressed as counts per minute (cpm) and as stimulation indexes (SI = cpm of cultures with drug/cpm of cultures without drug). Results were considered positive when SI was higher than 2.
LYMPHOCYTE PROLIFERATION IN THE PRESENCE OF A PROSTAGLANDIN INHIBITOR
A modification to the lymphocyte proliferative assay, consisting of the addition of a prostaglandin inhibitor (PI; indomethacin 1 μg/ml) to the cultures stimulated with drugs was simultaneously applied to patients and controls. The rationale for this approach has been published elsewhere.17 Activated monocytes in cultures of PBMC can secrete prostaglandins, namely PGE2, that inhibit the lymphocyte proliferative responses to various antigens in vitro.23 ,24 Several studies have shown that it is possible to restore the proliferative response by adding prostaglandin inhibitors to the cultures.25 ,26
Results were expressed as cpm and SI (SI = cpm of cultures with drug and PI/cpm of cultures with drug and without PI).
MITOGEN INDUCED LYMPHOCYTE PROLIFERATION
Responses to mitogens (phytohaemagglutinin (PHA) 10 μg/ml and pokeweed mitogen (PWM) 2.5 μg/ml) were performed in patients and controls in order to assess the adequacy of the culture system.27
EVIDENCE FOR PPSC IN VITRO AND CLINICAL CHARACTERISTICS
The possible associations between the presence of PPSC in vitro and the clinical characteristics of patients were analysed. These included age, sex, clinicolaboratory characteristics, presence of eosinophilia, pharmacological groups, latency time, remission time, and severity of the hepatitis as assessed by the maximal concentration of bilirubin, alkaline phosphatase, γ-glutamyltranspeptidase, and aminotransferases.
STATISTICAL ANALYSIS
The unpaired t test was used to assess statistical significance of differences observed in the means of continuous variables. The χ2 test and Fisher’s exact test were used to compare dichotomous variables. For non-parametric variables the Mann-Whitney U test was used. Statistical significance was considered at a p value of 0.05.
Results
Analysis of lymphocyte proliferative responses to PHA and PWM did not show any significant differences between patients and controls, indicating that non-specific T cell mediated immune responses were not affected in patients (data not shown).
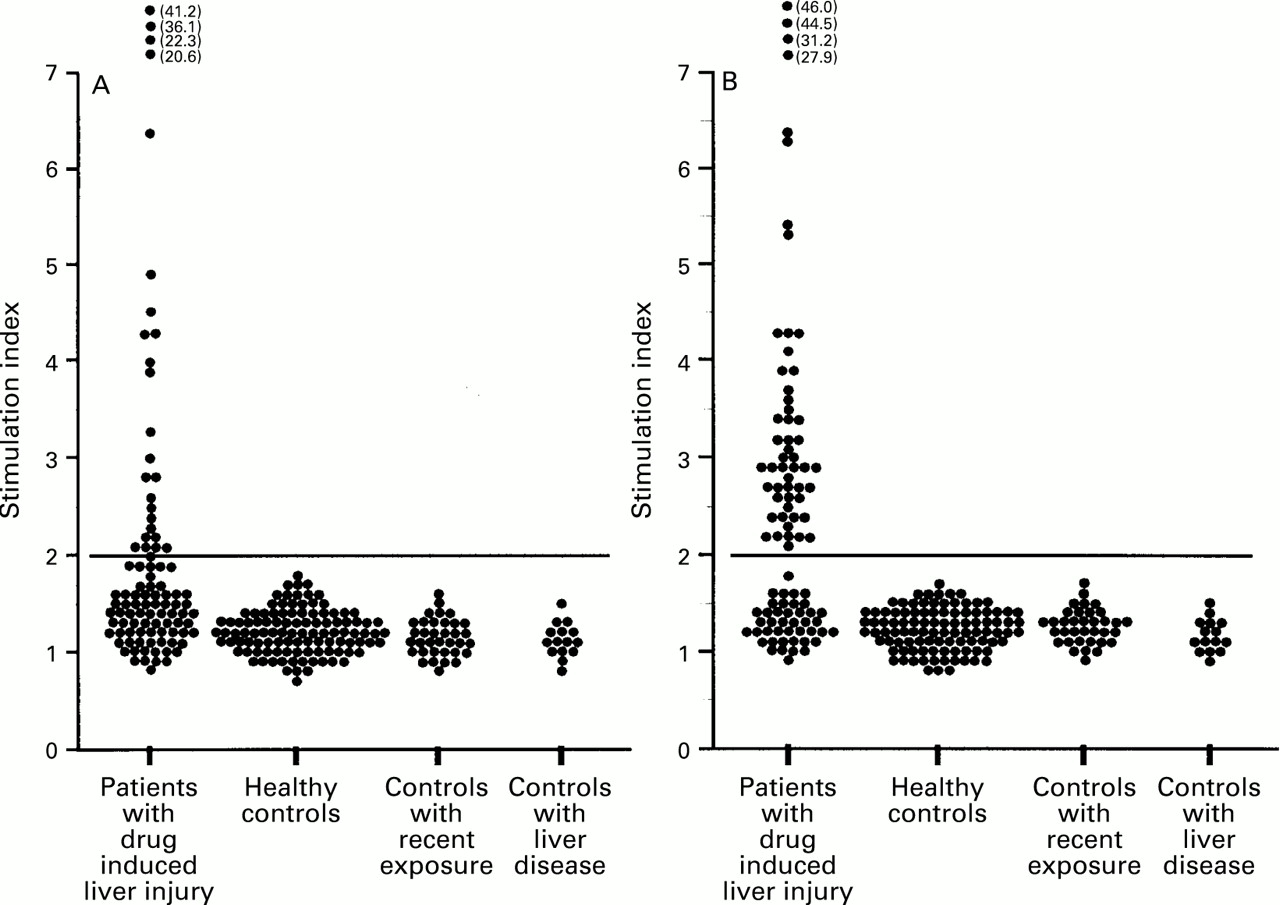
Figure 1 shows the stimulation indexes of lymphocyte proliferative responses to drugs in patients and controls. For each patient, the stimulation index represented corresponds to the higher lymphocyte response observed in the five different concentrations of the drug tested. Part A of the figure shows the stimulation indexes observed in standard conditions—that is, lymphocyte cultures with drugs alone. Significant proliferative responses to drugs (SI>2) were seen in 25 (26%) patients with a clinical diagnosis of drug induced liver injury. In these positive cases, stimulation indexes ranged from 2.1 to 41.2. The four cases with higher stimulation indexes correspond to cases of pyritinol induced prolonged cholestatic hepatitis. It is worth noting that no significant reactivity was found in the three types of controls studied. Part B of the figure shows the stimulation indexes observed when a prostaglandin inhibitor was added to the lymphocyte cultures. Positive results (SI>2) were observed in 53 (56%) patients with a clinical diagnosis of drug induced liver injury. Thus, a significant number of positive cases (n=28) was found only after use of this method. In most cases, an increase in the stimulation indexes was observed when a prostaglandin inhibitor was added to the cultures, even in cases already positive in standard conditions. A notable exception to this phenomenon was observed in the group of non-steroidal anti-inflammatory drugs (NSAIDs).

{kind=link}
: Lymphocyte stimulation indexes in patients and controls (A) in the presence of the suspected drug and (B) in the presence of the suspected drug and a prostaglandin inhibitor. The numbers in brackets represent the stimulation indexes of cases that fall outside the scale. The horizontal line represents the level of stimulation index above which results are considered positive.
Table 5 lists the drugs to which specific T cell reactivity was detected. The total number of drugs studied was 152, corresponding to a mean of 1.6 drugs per patient, with limits between 1 and 6. In all cases there was agreement between the drugs identified by immunological studies and the drugs suspected after a standard clinical imputation process was applied.28 In cases in which two or more drugs were equally suspected by clinical assessment, lymphocyte reactivity was found to one drug only. In three cases of cotrimoxazole induced hepatitis, lymphocyte reactivity was tested both to sulphamethoxazole and trimethoprim, and in all cases reactivity was observed only to sulphamethoxazole. In another case of erythromycin induced cholestatic hepatitis, in which the patient had been exposed successively to different salts of erythromycin, lymphocyte reactivity was tested against ethylsuccinate, estolate, and lactobionate, as well as to base erythromycin; lymphocyte sensitisation was detected only to lactobionate.
Drugs to which specific T cell reactivity was detected
In five cases, lymphocyte proliferative responses to the suspected drug were detected on two different occasions (table 6). In three cases the reactivity decreased and in two no changes were observed.
Cases of drug induced liver injury studied on two different occasions
Table 7 presents the possible associations between the presence of PPSC in vitro and the clinical characteristics of patients. Statistically significant differences were found between cases with and without evidence of PPSC when considering duration of latency (p=0.014) and remission (p=0.013), severity of hepatitis as assessed by alanine aminotransferase (p=0.027) and aspartate aminotransferase (p=0.012) concentrations, and the pharmacological groups of the drugs inducing hepatitis (p=0.017).
Clinical and laboratory features and their relation to the presence or absence of prostaglandin producing suppressor cells (PPSC) in vitro
Cases with evidence of PPSC had a significantly lower median latency period (11 days) than cases without PPSC (15 days) as assessed by the Mann-Whitney U test (p=0.042). The median duration of remission was also lower in the first group (43 v 65 days) although this did not reach statistical significance (p=0.146).
Table 8 shows the global results of specific T cell reactivity to drugs tested in 95 patients with a clinical diagnosis of drug induced liver injury, using different methods. It is worth noting that the addition of a prostaglandin inhibitor to the lymphocyte cultures increased significantly the ability to detect lymphocyte reactivity to drugs. The results obtained in a series of 25 cases previously published18 in which ex vivo drug antigens were used instead of the parental drug are also shown in table 8 for comparison. Although the percentage of positive cases with this approach was only 28%, several of these cases were not detected when the test was done in standard conditions or with simple addition of a prostaglandin inhibitor. Finally, in cases where the three different approaches were simultaneously applied—that is, lymphocyte proliferation to drugs alone, lymphocyte proliferation to drugs in the presence of a prostaglandin inhibitor, and lymphocyte proliferation to ex vivo drug antigens, a much higher percentage of positive cases was observed (88%).
Comparison of results observed in lymphocyte stimulation tests (LST) with drugs (standard), with drugs and a prostaglandin inhibitor (PI), and with ex vivo drug antigens (EVDA)
In order to assess whether a positive in vitro test was associated with the presence of extrahepatic manifestations which are usually considered to be a clinical marker of an immunological mechanism for drug hepatotoxicity, we analysed the frequency of these extrahepatic manifestations in patients with positive and negative test results. No significant differences were found, as assessed by Fisher’s exact test.
Discussion
Specific T cell reactivity to drugs has been used in an attempt to improve diagnosis of drug induced liver injury but a low sensitivity of the test has been reported.14 ,15 Most studies investigated individual cases or small series. We have analysed the value of this method in a large series of well characterised patients, subject to long follow up periods. We used modifications to the standard tests, in an attempt to overcome some of the problems that could theoretically explain the low sensitivity of the test—namely, the presence of prostaglandin producing suppressor cells in the in vitro culture system.17 ,23 ,29 Our results showed that this modification increased significantly the sensitivity of the test, without decreasing its specificity. In fact, no reactivity was found in any of the three types of controls studied. Control subjects with recent exposure to the suspected drugs without adverse effects are particularly important in this kind of study, because sensitisation to the drug could be an epiphenomenon observed in those exposed to the drug and unrelated to the hepatic lesion. Conversely, some liver diseases could somehow alter the immune system and predispose to non-specific sensitisation to drugs. Negative results observed in our controls with liver diseases unrelated to drugs exclude this possibility.
The use of a large number of concentrations of the drug seems to be of considerable importance, because in several cases lymphocyte reactivity was detected only to one or two concentrations of the drug. This finding is not totally unexpected as the optimal concentration of the drug for generating the adequate antigenic presentation in vitro is unknown. Furthermore, it is worth noting that the optimal concentration of a certain drug varies from one person to another. Therefore, the criteria of choosing a concentration corresponding to the average plasma therapeutic concentration of the drug and two concentrations above and two below that level are clearly arbitrary, although it was shown to be of practical importance in the sense that an optimal concentration could be either below or above the chosen reference concentration.
As suggested in our early studies,16 ,17 the increase in lymphocyte proliferation in response to drugs by the addition of a prostaglandin inhibitor to the cultures suggests that it is the presence of prostaglandin producing suppressor cells that prevents lymphocyte sensitisation to drugs being detected in standard conditions. This in vitro phenomenon seems to be clinically relevant in vivo, in the sense that patients in which this phenomenon was detected had a less severe disease, as assessed by aminotransferase concentrations and more rapid cure. This observation is interesting in view of the data showing a protective role of prostaglandins, namely PGE2, in experimental models of liver injury,30 as well as in patients with fulminant hepatic failure.31 Recent studies have shown that PGE2profoundly inhibits the synthesis of interleukin 2 and interferon γ,32 ,33 two lymphokines associated with the Th1 pattern, but not of interleukin 4 and interleukin 10 secreted by Th2 cells. There is growing evidence that the Th1 subset may be involved in organ specific autoimmune diseases, not only in animal models,34 but also in humans, as is the case in multiple sclerosis35 and rheumatoid arthritis.36 Many cases of drug induced prolonged cholestasis associated with the vanishing bile duct syndrome show some features in common with autoimmune liver diseases, such as primary biliary cirrhosis (PBC).37 ,38 It has been shown that biliary epithelial cells from patients with PBC exhibit aberrant expression of HLA class II antigens39 in association with T cell autoreactivity against biliary autoantigens,40 and this abnormal expression could be dependent on interferon γ.41 ,42Thus, it is tempting to speculate that, by inhibiting interferon γ and favouring a switch from the Th1 to the Th2 subset, PGE2may have an important role in preventing drug induced autoimmune liver disease.
An additional factor that could contribute to the high rate of detection of sensitised T cells in our series may be related to the rigorous and strict criteria we used in establishing the diagnosis of drug induced liver injury. Furthermore, we believe that in our series cases of liver damage induced by dose independent idiosyncratic metabolic mechanisms are under-represented.
Antihypertensives and some antimicrobial drugs seem to be more prone to inducing prostaglandin producing suppressor cells than other pharmacological groups. The inability to detect this phenomenon in the NSAID group is probably because these drugs are already prostaglandin inhibitors and therefore no additional effect is obtained with the addition of indomethacin.
We do not question the usual practice of diagnosing drug induced liver injury by clinical criteria, with emphasis on the exclusion of alternative causes and the establishment of a consistent temporal relation between drug intake and the onset of clinical manifestations.2 However, in patients exposed to more than one drug and particularly for recently marketed drugs, the demonstration of specific T cell reactivity to a given compound represents additional evidence in favour of its involvement in the induction of liver injury6 and is also important for defining the type of mechanism involved.
It is usual clinical practice to assume that the presence of clinical manifestations such as rash, arthralgia, and eosinophilia is the best marker for an immunological mechanism in drug induced hepatotoxicity.4 The fact that such clinical markers were absent in about 70% of our patients with a demonstrable T cell reactivity to drugs challenges this view. Furthermore, our results showing lymphocyte sensitisation to drugs in as many as 65% of the patients suggest that immunological mechanisms are much more frequent in drug hepatotoxicity than previously assumed.7 However, this does not preclude the possibility of coexistence of metabolic idiosyncratic mechanisms that could be responsible for the formation of reactive metabolites involved in the induction of the abnormal immune response.
Cross reactivity between drugs from the same pharmacological group often occurs and it is normally recommended that a patient with hepatitis associated with a given drug should avoid taking any drug belonging to the same group.43 However, our preliminary results on this topic suggest that drug sensitisation seems to be highly specific. In fact, in several cases in which patients had been exposed to pharmacologically related compounds or even to different salts of a given drug, lymphocyte reactivity was detected only to one drug or to a particular drug salt. Furthermore, in the rare instances (five cases) in which patients had been tested more than once within a period of few weeks after the onset of the clinical sysptoms, reactivity was always detected to the same drug. Taken together, these data clearly show the high specificity of these in vitro tests.
The notable increase in the sensitivity of drug specific T cell reactivities obtained with this new approach, together with its high specificity, could lead to a recommendation for the more general use of these tests in clinical practice.44 The only limitation to such widespread use is that the relative complexity of this method implies that such tests should be confined to specialised laboratories with experience in in vitro functional cellular immunology techniques. However, the renewed interest in drug induced liver injury and the importance of more accurate diagnoses probably justifies the effort required of specialised laboratories to make such tests available in the investigation of selected cases of drug induced hepatitis.
In conclusion, modified lymphocyte transformation test used in our study significantly increased our ability to detect lymphocyte sensitisation to drugs without altering the specificity of the test. We therefore suggest that the study of specific T cell reactivity to drugs should have a place in the diagnosis of drug induced liver injury, particularly in patients exposed to more than one drug.
Acknowledgments
This project was supported in part by grants from JNICT (Junta Nacional de Investigação Científica e Tecnológica, Lisbon, Portugal) to RMMV.