Article Text

Abstract
Background and aims: Impaired accommodation and hypersensitivity to distension of the proximal stomach are considered to be important factors in the pathogenesis of dyspeptic complaints. As fundus relaxing agents may be effective in the treatment of these symptoms, insight into the mediators involved in fundic accommodation and associated perceptual responses is important. Therefore, we studied the effect of nitric oxide (NO) synthase inhibition by NG-monomethyl-l-arginine (l-NMMA) on fundic tone, postprandial sensations, and gastric perception in healthy volunteers.
Subjects and methods: Eighteen healthy volunteers participated in a double blind, placebo controlled, randomised study. They underwent a gastric barostat study to evaluate the effect of l-NMMA on meal and distension induced sensations and on fundic relaxation in response to oral meal intake, intraduodenal lipid, and glucagon administration.
Results: Compared with placebo, l-NMMA decreased fundic volume after oral meal intake (438 (55) v 304 (67) ml; n=8; p<0.05) and during intraduodenal lipid infusion (384 (37) v 257 (43) ml; n=10; p<0.05) but not after glucagon injection (570 (62) v 540 (52) ml; n=4; p=0.4). In addition, basal fundic volume was significantly reduced by l-NMMA. Scores for nausea and satiation were decreased by l-NMMA after oral meal intake but not during intraduodenal lipid infusion. Perception scores to gastric distension were not altered by l-NMMA.
Conclusions: NO is involved in maintaining basal fundic tone and in meal induced fundic relaxation in humans, but not in visceral perception.
- nitric oxide
- nitric oxide synthase
- gastric accommodation
- visceral perception
- barostat
- NO, nitric oxide
- l-NMMA
- NG-monomethyl-l-arginine
- MDP, minimal distending pressure
- VAS, visual analogue scale
Statistics from Altmetric.com
- NO, nitric oxide
- l-NMMA
- NG-monomethyl-l-arginine
- MDP, minimal distending pressure
- VAS, visual analogue scale
Normal digestion and perception of sensations associated with meal intake are dependent on a reflex relaxation of the proximal stomach initiated by food ingestion. This so-called gastric accommodation reflex allows storage of the meal without a concomitant increase in intragastric pressure. Impaired relaxation of the proximal stomach may contribute to the development of meal induced symptoms in conditions such as functional dyspepsia, diabetes mellitus, postfundoplication syndrome, rumination, postsurgical gastroparesis, and diabetic gastroparesis.1–,5 Pharmacological interventions aimed at relaxing the proximal stomach may be effective in conditions characterised not only by impaired gastric accommodation but also by increased sensitivity to gastric distension, as seen for example in patients with functional dyspepsia.6 This has been suggested previously in studies using the 5-HT1 agonist sumatriptan, which was shown to increase meal induced gastric relaxation, to increase the threshold for discomfort during gastric distension in healthy volunteers, and to increase caloric intake in dyspeptic patients.1,7 Therefore, to develop fundus relaxing drugs, insight into the mediators involved in the regulation of proximal gastric tone and associated perceptual responses is important.
Nitric oxide (NO) is recognised as an important neurotransmitter in the human gut, mediating a variety of motility patterns.8–,10 Animal studies have provided abundant evidence that both basal fundic tone and relaxation of the proximal stomach induced by vagal stimulation, meal ingestion, or intraduodenal lipid are mediated by NO.11–,17 In addition, evidence is available that NO is involved in the modulation of visceral perception, for example from rat experiments, showing that intraperitoneal injection of acetic acid results in an increase in nitrergic neurones in specific regions of the brain.18 Also, NO synthase immune reactivity has been demonstrated in lumbosacral afferents and preganglionic neurones innervating the pelvic viscera.19
Data illustrating a role for NO in human proximal gastric motility and perception are limited to in vitro studies10 or to in vivo studies investigating the effect of NO donors such as nitrates.20–,22 However, to gain more insight into the role of endogenous NO, studies evaluating the effect of an NO synthase inhibitor are required. We previously demonstrated that the selective NO synthase inhibitor NG-monomethyl-l-arginine (l-NMMA) dose dependently affects small intestinal and oesophageal motility, illustrating that this chemical is a useful tool to investigate the role of endogenous NO in humans.8,9,23 Therefore, in the present study, we investigated the effect of l-NMMA in healthy volunteers on basal fundic volume and fundic relaxation. In addition, perception of fundic distension and meal induced sensations were assessed.
SUBJECTS AND METHODS
Subjects
Eighteen healthy male volunteers (mean age 24 years, range 19–30) were studied. All subjects were free of gastrointestinal symptoms, with no previous gastrointestinal surgery, and were not taking any medications. Subjects were studied after an overnight fast and were not allowed to smoke or drink alcohol for at least 24 hours before the study. All volunteers gave written informed consent to participate in the study which was approved by the medical ethics committee of the Academic Medical Centre, Amsterdam.
Methods
Gastric barostat
The barostat allows continuous recording of proximal gastric volume using an intragastric bag set at a fixed pressure level. In addition, gastric sensitivity can be assessed by distending the intragastric bag. Following anaesthesia of the throat (10% xylocaine spray), subjects swallowed a 1200 ml polyethylene bag, tightly wrapped on the distal end of a double lumen polyvinyl tube (Salem Sump tube, Sherwood Medical St Louis, USA; outer diameter 4 mm). The bag was unfolded by inflating it with 500 ml of air and was positioned in the proximal stomach by gently pulling the catheter back. The catheter was connected to an electronic barostat that automatically corrected for the compressibility of air (Medtronic Functional Diagnostics, Stockholm, Sweden). Recorded data were stored on a personal computer using commercially available software (Polygram for Windows, Medtronic Functional Diagnostics, Stockholm, Sweden).
Intraduodenal infusion
Study II. A polyurethane nasoduodenal feeding tube was placed for lipid infusion (Flocare, Chåtel Medical Devices SA, Switzerland; length 125 cm, outer diameter 3.3 mm). The catheter, containing a guidewire in the central lumen, was positioned 30 cm beyond the pyloric region, under fluoroscopic control. The guidewire was then removed and the catheter was connected to a perfusion pump. Based on previous studies,24 a 10% lipid solution (Intralipid, Pharmacia and Upjohn, the Netherlands; energy load 1.1 kcal/ml) was infused at a rate of 1 ml/min.
Sensation scores
Sensations of bloating, nausea, pain, and satiation were assessed individually, using a 10 cm continuous visual analogue scale (VAS: 0 cm=no sensation, 10 cm=worst ever). Perception of sensations induced by feeding was scored just before and at five minute intervals after meal intake or following the start of intraduodenal infusion of lipid (study I and II, respectively). Sensations perceived during gastric distension (study II) were scored halfway through each distension step, both during fasting and during intraduodenal infusion of lipid.
Drugs
l-NMMA (NG-monomethyl-l-arginine monoacetate) was supplied by Alexis Corporation (Switzerland) and donated by a generous grant from the Janssen Research Foundation (Belgium). l-NMMA was dissolved in a sterile 0.9% NaCl solution to a concentration of 15 mg/ml. Equal volumes of the vehicle were used in the control studies. Glucagon (GlucaGen; glucagon hydrochloride) was supplied by Novo Nordisk Pharma (the Netherlands).
Experimental protocols
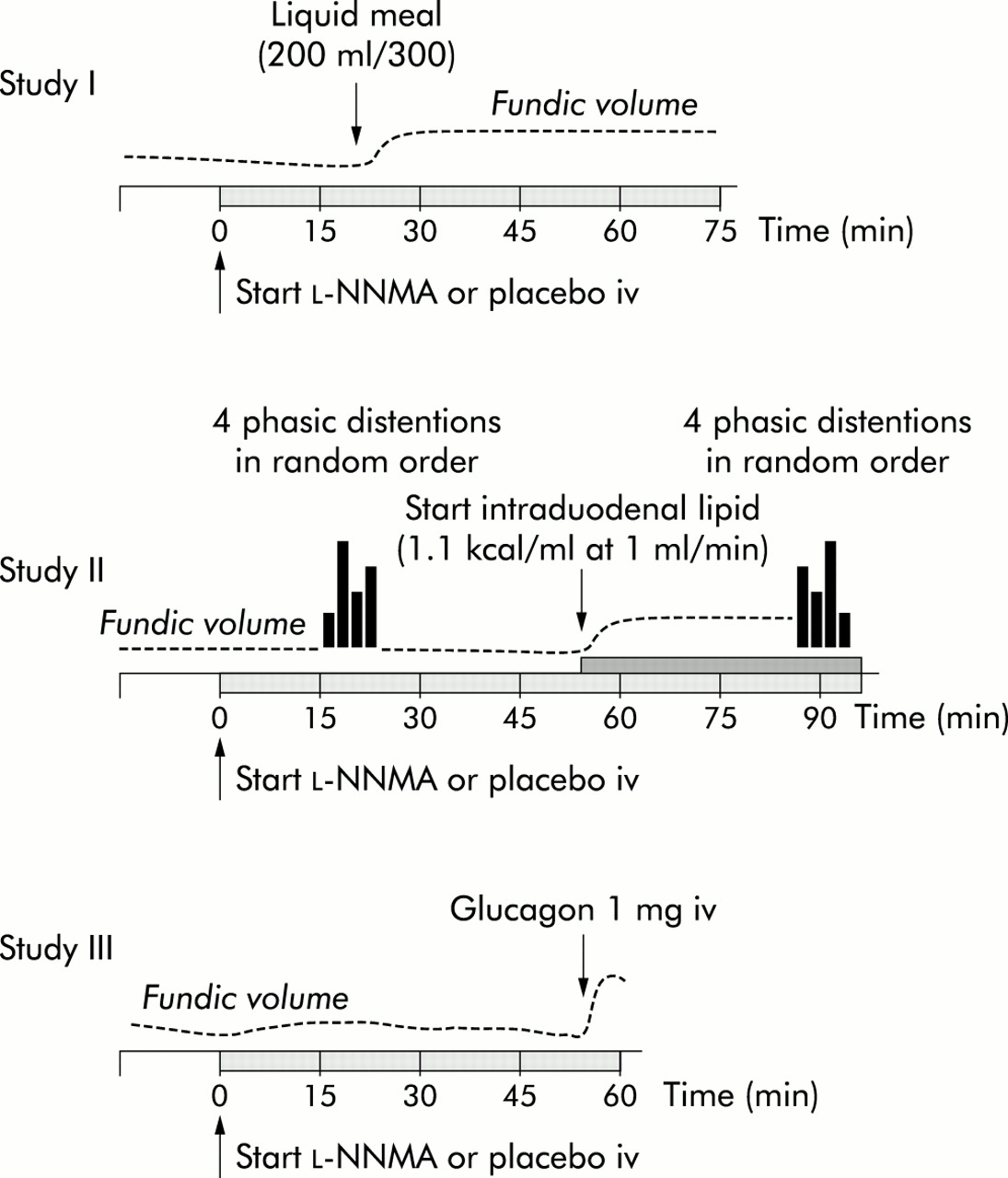
Three study protocols were used (see fig 1⇓). Of the 18 volunteers, three participated in studies I and II and three participated in studies II and III. Therefore, the total number of subjects studied was 10 for study I, 10 for study II, and four for study III. All studies were designed in a double blind placebo controlled manner, performed on two separate days at least three days apart. Study I was designed to investigate the effect of l-NMMA on fundic relaxation after oral intake of a liquid caloric meal. In addition, sensations evoked by the test meal were studied. In study II, subjects received lipids intraduodenally via a nasoduodenal feeding tube. We chose this approach (1) to bypass the possible effects of NO synthase inhibition on gastric emptying and (2) to create a situation of increased sensitivity to gastric distension, as described previously.24 The effects of l-NMMA on sensations induced by duodenal lipid and by gastric distension were studied before and during intraduodenal administration of lipids. In addition, we studied fasting fundic volume and fundic relaxation induced by intraduodenal lipid. Study III was designed to evaluate a possible postjunctional effect of l-NMMA. Therefore, in study III, we evaluated the effect of l-NMMA on basal volume and fundic relaxation after glucagon administration, known to relax the proximal stomach, probably via a direct NO independent mechanism.25
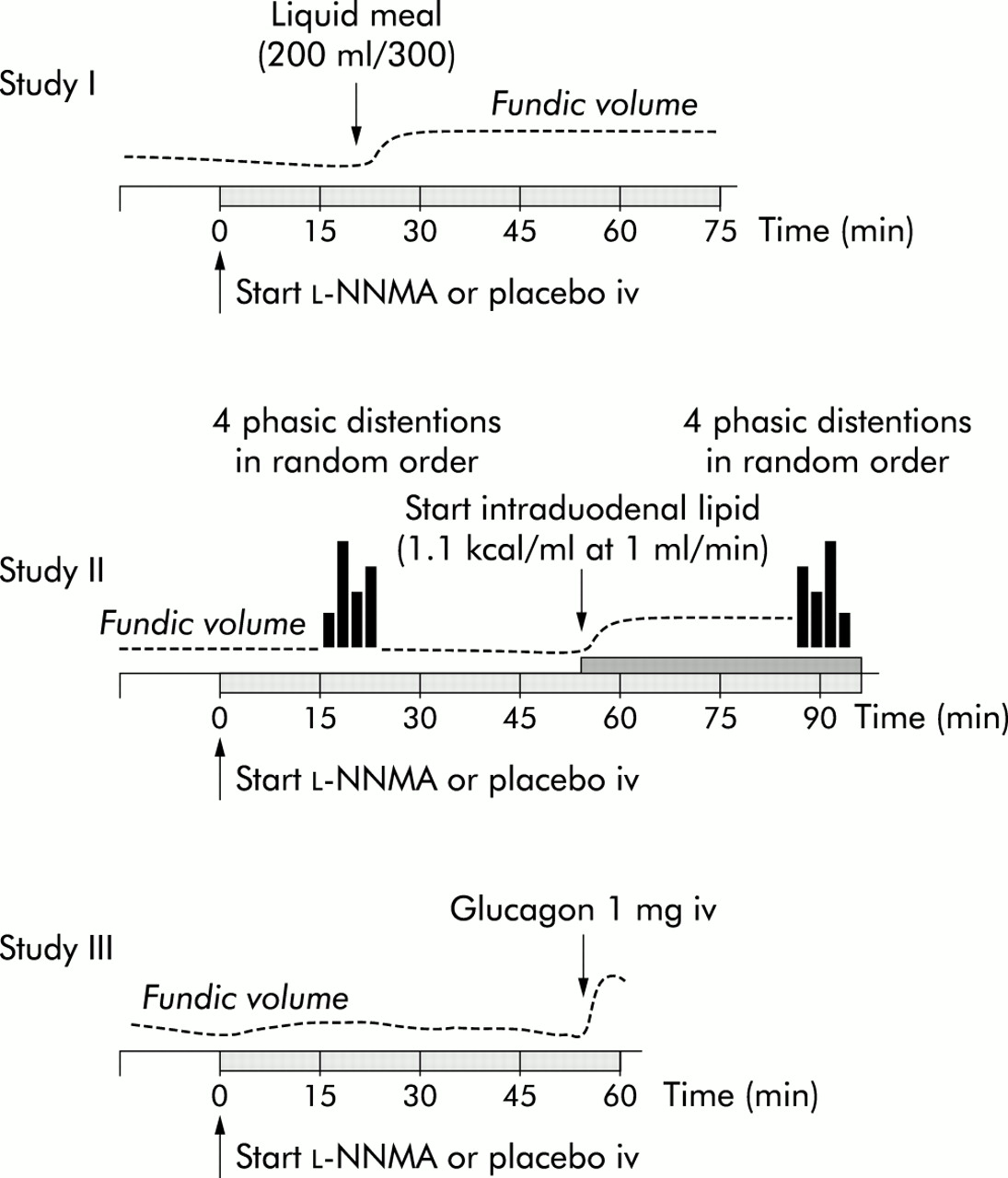
Schematic representation of the study protocols (see text for detailed descriptions of the different studies).
Study I: fundic accommodation and sensations after oral meal intake
In this study, both proximal stomach and antropyloroduodenal motility were recorded by combining a gastric barostat test with antropyloroduodenal manometry. However, for clarity, the manometry data are presented in a separate paper.26
Subjects reported to the laboratory at 7:45 am. The barostat bag was positioned in the proximal stomach as described above. An intravenous line was placed in the left arm for infusion of either placebo or l-NMMA. Heart rate, and systolic and diastolic blood pressures were measured every 10 minutes during the protocol using an automatic sphygmomanometer (Boso, Jungingen, Germany). After an equilibration period of 30 minutes, minimal distending pressure (MDP) was determined as the minimum pressure at which balloon volume was >30 ml. Baseline operating pressure was set at MDP+2 mm Hg. Intragastric bag volume was recorded under basal conditions over 15 minutes. l-NMMA was infused intravenously at a rate of 12 mg/kg over five minutes (bolus) followed by maintenance infusion of 6.7 mg/kg/h (fig 1⇑). In the control studies, an equal volume of saline was infused at equal rates. Twenty minutes after the start of the infusion, 200 ml of a liquid test meal (Nutridrink, Nutricia Zoetermeer, the Netherlands; energy load 300 kcal) was consumed with the aid of a straw. Fundic volume was recorded over the following 60 minutes. Postprandial sensations were scored every five minutes.
Study II: fundic tone and sensations before and after intraduodenal lipid
Subjects reported to the laboratory at 7:45 am. After placement and positioning of the nasoduodenal catheter and the barostat bag, an intravenous line was placed and an equilibration period of 30 minutes was allowed. Thereafter, MDP was determined as described above. Operating pressure was set at MDP+2 mm Hg and baseline intragastric bag volume was recorded for 15 minutes. Intravenous administration of either l-NMMA (bolus of 12 mg/kg over five minutes, followed by maintenance infusion of 6.7 mg/kg/h) or placebo was then started (fig 1⇑). Basal volume during the first 15 minutes of infusion was recorded, followed by a series of four isobaric distensions at 3, 6, 9, and 12 mm Hg above MDP, in random order. Each pressure step lasted 60 seconds, with 120 second intervals at the level of MDP. Perception scores were assessed at each pressure step. Again, operating pressure was set at MDP+2 mm Hg and continuous intraduodenal lipid infusion was started 30 minutes after the first distension series. Perceived meal related sensations were scored every five minutes during lipid infusion. A second series of four random isobaric distensions at MDP+ 3, 6, 9, and 12 mm Hg was performed 30 minutes later while continuously infusing lipids, and perception scores were assessed at each distension level. Heart rate and blood pressure were measured every 10 minutes.
Study III: glugacon induced fundic relaxation
Subjects reported to the laboratory at 8:00 am. Placement of the barostat bag, equilibration, determination of MDP, and baseline volume recording (15 minutes) were performed as described above. The same dose of l-NMMA was used as in the previous two studies. Similar to study II, fasting fundic volume was recorded for 55 minutes (fig 1⇑). At t=55 minutes, subjects received 1 mg of glucagon intravenously, flushed with 5 ml of saline, in the right forearm. Heart rate and blood pressure were measured every 10 minutes.
Data analysis
Fundic volume
Study I
Basal volume 15 minutes before and 20 minutes after the start of infusion (l-NMMA or placebo) was determined as mean volume over the given period. Meal induced relaxation was expressed as mean volume over the 60 minutes after the meal. Volume change (or ΔV) was determined as the difference between mean basal volume (before infusion) and mean postprandial volume. Based on previous studies, a volume change of >64 ml was considered normal.1
Study II
Basal volume was measured 15 minutes before and 15 minutes after the start of infusion of l-NMMA or placebo. In addition, basal volume was measured between 40 and 55 minutes after the start of infusion (that is, 15 minutes after the first distension series). Lipid induced relaxation was expressed as mean volume over 30 minutes after the start of intraduodenal infusion of lipid. ΔV was determined as the difference between mean basal volume (before infusion) and mean postprandial volume.
Study III
Similar to study II, basal volume was measured 15 minutes before and 15 minutes after the start of infusion of l-NMMA or placebo and between 40 and 55 minutes after the start of infusion. Fundic relaxation in response to glucagon administration was determined as mean volume over five minutes following injection. ΔV was determined as the difference between mean basal volume (before infusion) and mean volume after glucagon.
Fundic compliance
Study II. Gastric distension was performed at fixed pressure levels (3, 6, 9, and 12 mm Hg) above MDP. The mean of the corresponding volumes over the last 30 seconds of each distension step was measured and plotted against the corresponding distending pressure. Fundic compliance was calculated as the slope of the pressure-volume curve, as described previously.1
Meal induced sensations
Following meal ingestion and the start of intraduodenal lipid administration (studies I and II, respectively), perceived sensations were scored every five minutes. Scores for bloating, nausea, pain, and satiation were analysed individually as repeated measures in time using a customised mixed effects model.
Sensation induced by gastric distension
Study II. We performed two series of four distensions at fixed pressure levels applied in random order: one during fasting and one during intraduodenal lipid administration (distension series 1 and 2, respectively). For each distension series, scores for bloating, nausea, pain, and satiation were plotted against the corresponding distending pressure.
Statistical analysis
For analysis of meal induced sensation scores, a mixed effects model was fitted using a standard software package (S-PLUS 2000). As each sensation score is dependent on the previous score, it is not possible to use standard techniques for statistical analysis such as t tests. Mixed effects models are similar to linear regression but account for the structure of the repeated measures using random effects.27 Random effects allow the intercept and the value of some other coefficients to vary from person to person. In our analysis of the data on meal induced sensations, we used a model that accounted for the time postprandial and the square of the time. The random effects were a constant and the gradient associated with time.
The model used to describe meal induced sensations perceived at time t by person i under treatment j, yijt was: where εijt ∼ N(0, σ2).
where εijt ∼ N(0, σ2).
Distension induced sensations were compared using a repeated measures ANOVA with the Greenhouse-Geisser correction, using a standard software package (SPSS 9.0). All other data were compared using a Student's t test (SPSS 9.0) and are presented as mean (SEM); p values <0.05 were considered statistically significant.
RESULTS
Effect of l-NMMA on blood pressure and heart rate
All subjects tolerated the studies well. In study I, mean diastolic blood pressure was significantly increased from 73 (2) mm Hg after placebo to 84 (2) mm Hg after l-NMMA infusion (p<0.01) whereas mean heart rate was significantly decreased from 69 (5) bpm (placebo) to 58 (3) bpm (l-NMMA) (p<0.01). In study II, diastolic blood pressure increased from 75 (1) mm Hg (placebo) to 82 (2) mm Hg (l-NMMA) (p<0.01) and heart rate decreased from 60 (2) bpm (placebo) to 54 (2) bpm (l-NMMA) (p<0.01). In study III, l-NMMA increased diastolic blood pressure from 69 (3) mm Hg (placebo) to 79 (4) mm Hg (p<0.05) and heart rate decreased from 58 (4) bpm (placebo) to 52 (3) bpm (p<0.05). Systolic blood pressure was not significantly altered by l-NMMA. Cardiovascular effects were sustained during the course of the studies. No side effects were reported.
Effect of l-NMMA on basal fundic volume and fundic relaxation
Basal fundic volume and fundic relaxation induced by oral meal intake (study I)
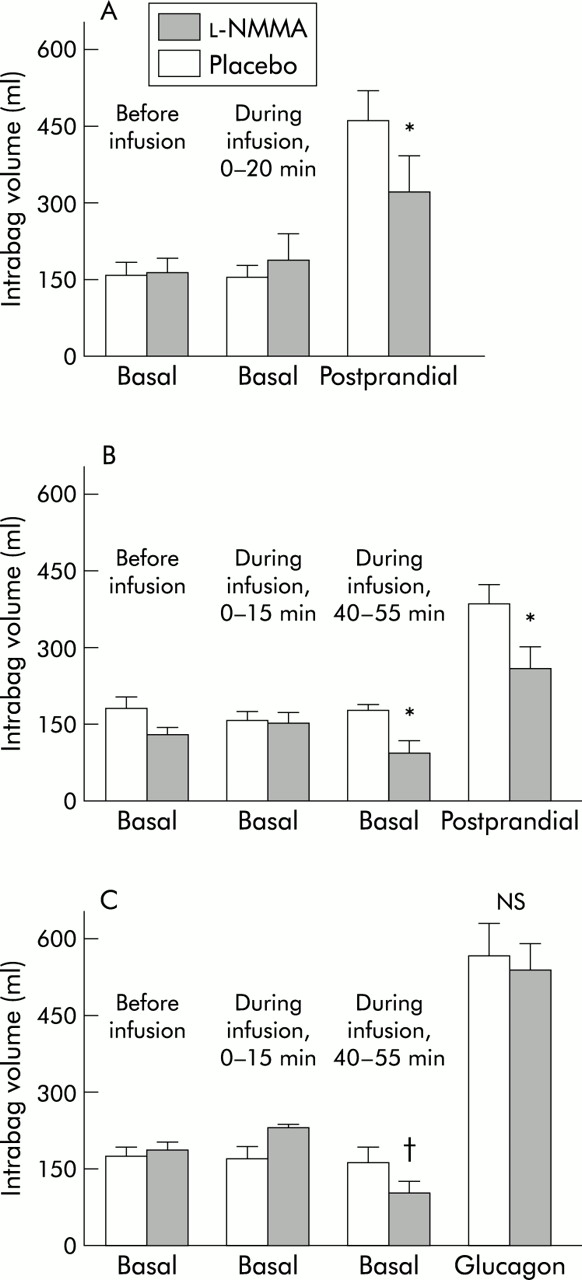
Mean fundic volume was similar before the start of placebo and l-NMMA (fig 2A⇓). l-NMMA did not significantly alter basal volume 20 minutes after the start of infusion (fig 2A⇓). In eight of 10 subjects, ingestion of the meal resulted in fundic relaxation that was considered normal (ΔV >64 ml) during placebo. Mean observed relaxation (or ΔV) in these individuals (n=8) decreased from 274 (35) ml (placebo) to 143 (55) ml (l-NMMA) but this did not reach statistical significance (p=0.08). In contrast, as shown in fig 2A⇓, mean postprandial volume was significantly decreased by l-NMMA compared with placebo.
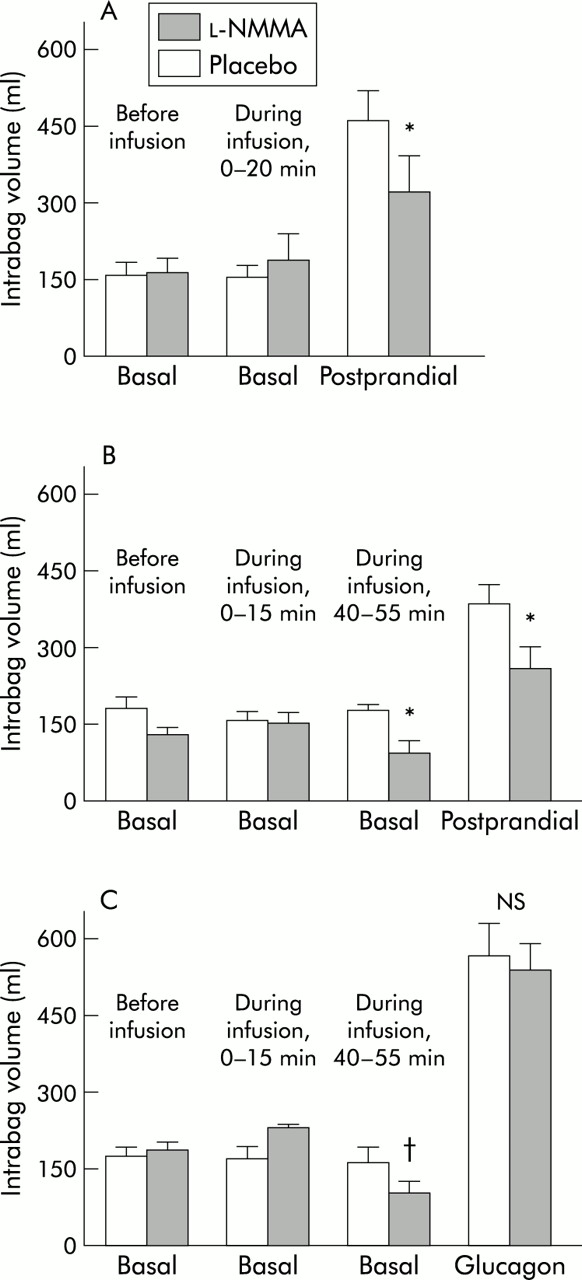
Effect of NG-monomethyl-l-arginine (l-NMMA) and placebo on basal and postprandial fundic volume (A) after oral ingestion of a liquid meal, (B) after intraduodenal infusion of lipid, and (C) after injection of glucagon. Data are mean (SEM). *p<0.05, paired t test versus placebo; †p<0.05 paired t test versus basal (before infusion).
Basal fundic volume and fundic relaxation induced by intraduodenal lipid (study II)
Baseline fasting fundic volume was similar before the start of placebo and l-NMMA (fig 2B⇑). l-NMMA did not significantly alter fasting volume during the first 15 minutes. However, l-NMMA gradually decreased fasting fundic volume during the course of the study which was statistically significant over the last 15 minutes before the start of intraduodenal lipid administration (40–55 minutes following the start of drug infusion) (fig 2B⇑). All (n=10) subjects showed marked fundic relaxation following the start of intraduodenal lipid which was significantly decreased by l-NMMA compared with placebo (ΔV: from 204 (32) ml to 129 (32) ml; p<0.05). In addition, mean postprandial volume was significantly decreased by l-NMMA compared with placebo (fig 2B⇑).
Basal fundic volume and fundic relaxation induced by glugacon (study III)
Baseline fasting fundic volume before the start of placebo or l-NMMA was comparable for both groups (fig 2C⇑). Similar to study II, l-NMMA did not significantly alter fasting volume during the first 15 minutes but significantly decreased mean fasting fundic volume over the last 15 minutes of the recording time, 40–55 minutes following the start of drug infusion (fig 2C⇑). Glucagon administration induced an instant and marked relaxation of the fundus in all (n=4) subjects which was not altered by l-NMMA (ΔV: 397 (71) ml and 356 (66) ml for placebo and l-NMMA, respectively; p=0.2). In addition, mean volume after glucagon was not significantly altered by l-NMMA compared with placebo (fig 2C⇑).
Effect of l-NMMA on visceral perception
Sensations after oral meal intake (study I)
At baseline, subjects reported comparable sensation scores (see fig 3⇓, t=0). Following the meal, subjects reported increased sensations of bloating, satiation, pain, and nausea. Scores for bloating and pain were not altered by l-NMMA whereas subjects reported significantly decreased scores for nausea and satiation during l-NMMA infusion compared with placebo (fig 3⇓).
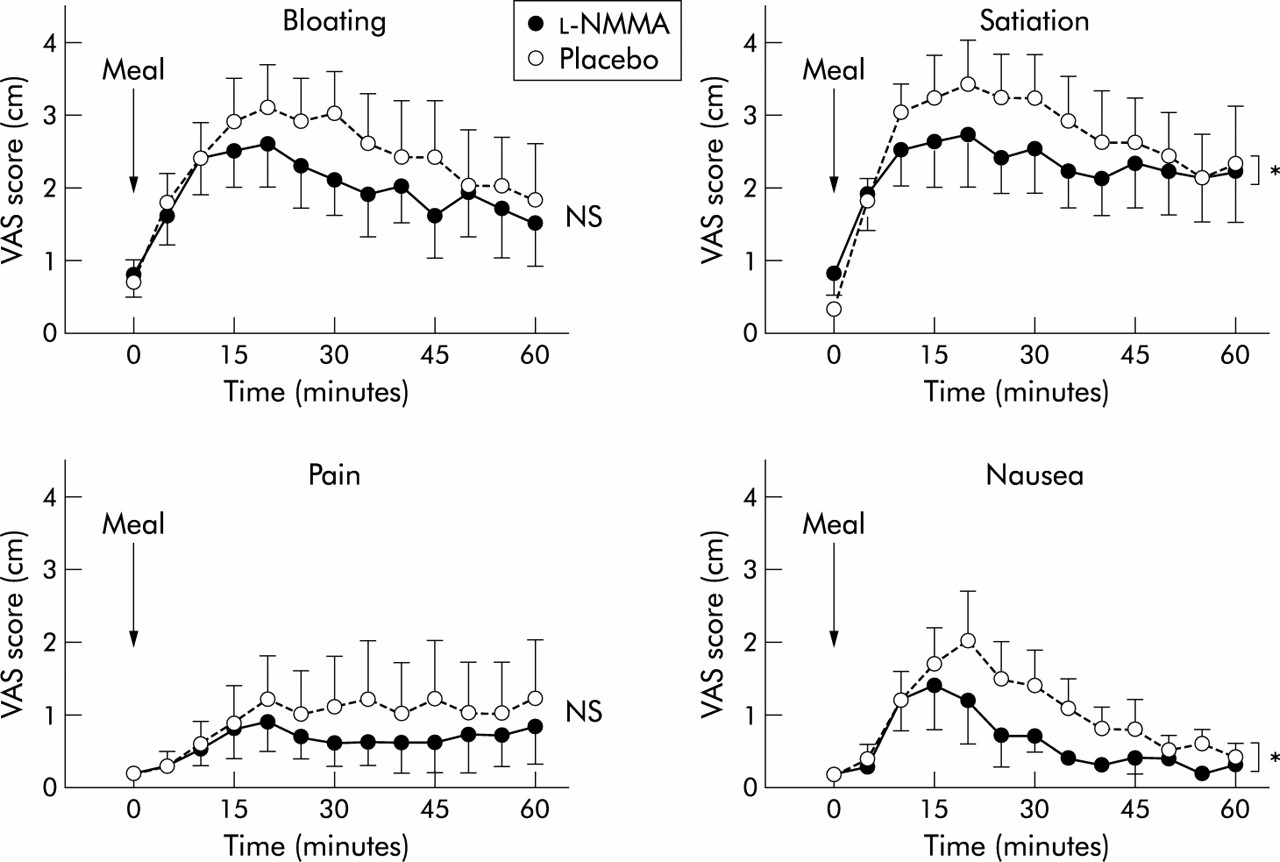
Effect of NG-monomethyl-l-arginine (l-NMMA) and placebo on sensation scores for bloating, satiation, pain, and nausea after oral ingestion of a nutrient liquid meal (study I). Visual analogue scale (VAS) scores for satiation and nausea after oral meal intake were significantly decreased by l-NMMA compared with placebo (*p<0.05, customised mixed model). Data are expressed as the observed rough mean (SEM).
Sensations after duodenal lipid infusion (study II)
Sensation scores were comparable before the start of intraduodenal lipid administration. No significant scores for nausea and pain were reported during intraduodenal administration of lipid, during both placebo and l-NMMA administration (maximum score for nausea: 0.6 (0.4) and 0.4 (0.3) cm, respectively; maximum score for pain: 0.3 (0.2) and 0.3 (0.1) cm, respectively). Although sensation scores for bloating and satiation tended to increase slightly during intraduodenal lipid, subjects perceived only very low scores, during both placebo and l-NMMA (maximum score for bloating: 1.4 (0.5) and 1.6 (0.7) cm, respectively; maximum score for satiation: 1.4 (0.6) and 1.4 (0.6) cm, respectively). l-NMMA did not significantly alter any of the sensation scores compared with placebo.
Sensation induced by gastric distension (study ii)
Subjects reported only mild sensations of pain and nausea during fundic distension while fasting. As shown in fig 4⇓, intraduodenal lipid tended to increase the perception of pain and nausea, although this did not reach statistical difference. Scores for bloating and satiation were more pronounced in both distension series and significantly increased during intraduodenal lipid compared with placebo (fig 4⇓). No significant effect on sensation scores during distension was seen between l-NMMA and control studies during both fasting and intraduodenal lipid infusion (fig 4⇓).

Effect of NG-monomethyl-l-arginine (l-NMMA) (filled symbols) and placebo (open symbols) on sensation scores for bloating, satiation, pain, and nausea in response to fundic distension during fasting and intraduodenal lipid infusion. Data are mean (SEM). MDP, minimal distending pressure.
Effect of l-NMMA on fundic compliance
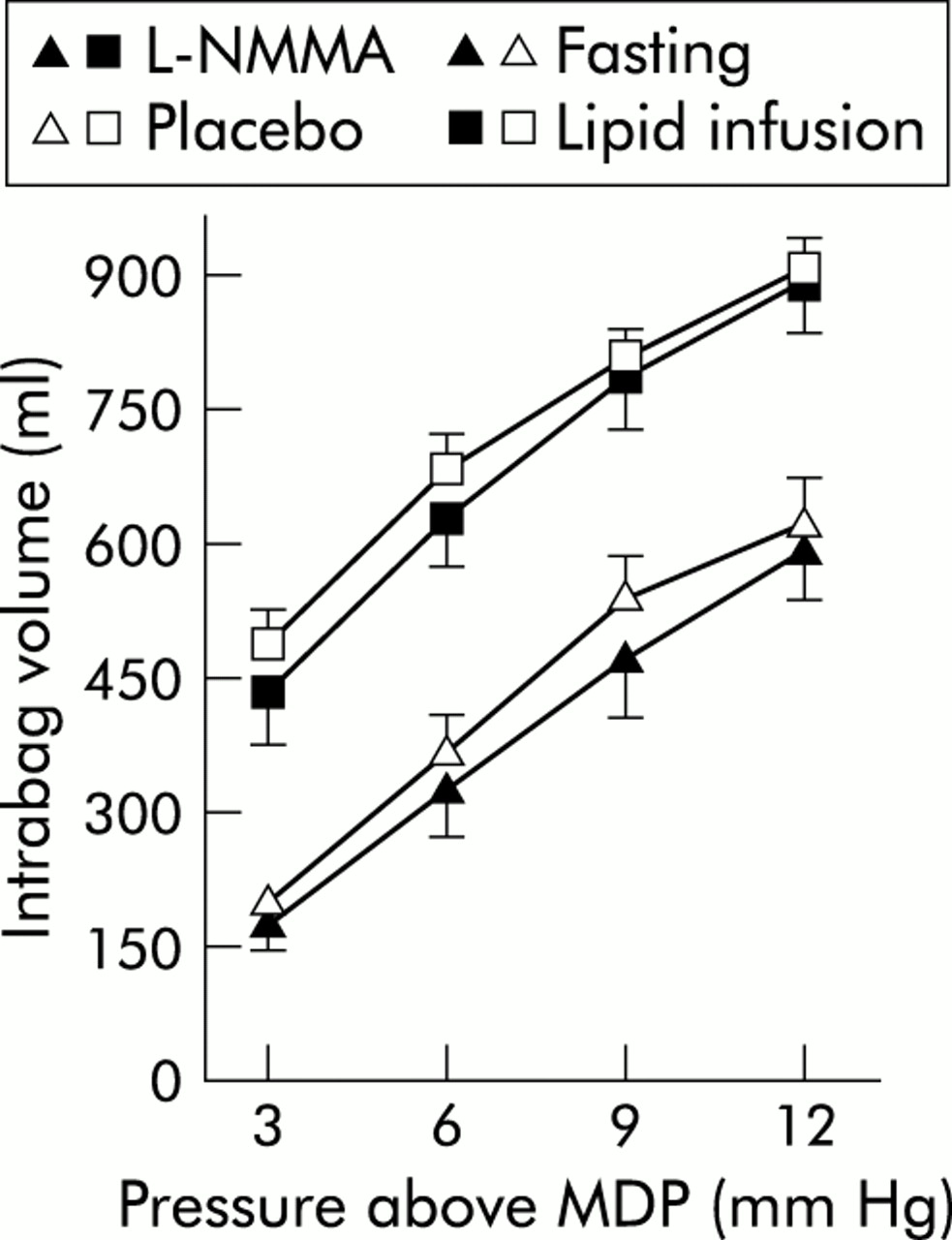
Fundic compliance during fasting was not significantly altered (placebo 50 (4) vl-NMMA 46 (6) ml/mm Hg). Likewise, during infusion of lipid, mean fundic compliance was not significantly affected by l-NMMA (placebo 46 (3) vl-NMMA 50 (5) ml/mm Hg). Pressure-volume curves are shown in fig 5⇓.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of NG-monomethyl-l-arginine (l-NMMA) (filled symbols) and placebo (open symbols) on pressure-volume curves in response to isobaric fundic distension during fasting and intraduodenal lipid infusion. MDP, minimal distending pressure.
DISCUSSION
In this study, we evaluated the effect of NO synthase inhibition by l-NMMA on proximal gastric volume and perception in healthy human subjects. We showed that l-NMMA decreased basal fundic volume and reduced fundic relaxation both after ingestion of a liquid meal and during intraduodenal lipid infusion, indicating that NO is involved in modulating fundic tone. Finally, no effect of l-NMMA on perception was seen, indicating that, at least in healthy volunteers, NO has no major role in visceral perception.
Animal studies have provided abundant evidence that both basal tone and relaxation of the proximal stomach, induced by vagal stimulation, meal ingestion, or intraduodenal lipid, are mediated by NO.11–,17 Similarly, we showed that NO synthesis inhibition by l-NMMA contracted the gastric fundus, resulting in a reduction in basal fundic volume. The effect was only observed after prolonged infusion of l-NMMA, most likely due to the time dependent inhibitory effect of l-NMMA on NO synthase activity.28 In addition, l-NMMA reduced fundic volume following ingestion of a nutrient liquid meal and during intraduodenal lipid. It should be emphasised that the reduction in postprandial volume observed during l-NMMA may simply reflect functional antagonism, resulting from the contractile effect of l-NMMA on basal tone. However, fundic relaxation induced by glucagon, known to act by a direct and NO independent mechanism,25 was not affected by l-NMMA. Therefore, we concluded that the reduction in postprandial volume by l-NMMA resulted from an effect on NO release, illustrating that NO is involved in meal induced relaxation of the human proximal stomach. These findings are in line with the recent in vitro study by Tonini et al demonstrating that relaxation of muscle strips of the human proximal stomach induced by nerve stimulation is inhibited by NO synthase inhibition.10
With respect to the site of action, l-NMMA may act at all possible levels as NO is found to act throughout the central nervous system and the enteric nervous system. The fact that fundic relaxation induced by glucagon was not inhibited by l-NMMA excludes a possible postjunctional effect on the fundic smooth muscle. In addition, we did not observe an effect of NO synthase inhibition on plasma pancreatic polypeptide concentrations,29 indicating that vagal efferent output was not altered by l-NMMA. Finally, no significant effect on reaction time was noted (data not shown), suggesting no sedative effect of l-NMMA. Thus although a central action of l-NMMA cannot be excluded under the current experimental conditions, these findings suggest that l-NMMA increases fundic tone by reducing nitrergic neuronal input at a peripheral level.
Impaired accommodation to a meal, as encountered in a number of clinical conditions, is considered an important pathophysiological mechanism responsible for dyspeptic complaints.1–,5 For example, in functional dyspepsia, impaired accommodation is associated with early satiety and weight loss.1 Therefore, we anticipated that reduction in gastric relaxation by l-NMMA should increase postprandial sensation scores. In contrast, scores for nausea and satiation were significantly decreased. As NO is also involved in the modulation of visceral sensation,18,30 this effect could result from interaction of l-NMMA with perception. However, no changes in perception of gastric distension were reported during fasting. Furthermore, when the stomach was distended during intraduodenal infusion of lipid, which is known to cause increased sensitivity in healthy subjects,24 no effect of l-NMMA was observed, excluding interference with visceral perception. The observation that during l-NMMA infusion subjects only reported decreased sensation scores after oral meal intake may therefore result from an effect of l-NMMA on gastric emptying. Alternatively, as gastric wall tension seems to be the major determinant of gastric perception,31 reduced perception of meal induced sensations may also be explained by the reduction in volume and the associated reduction in wall tension. The fact that healthy volunteers also experienced mild degrees of nausea and pain during the experiment probably reflects the artefact that is introduced by measuring meal induced sensations while having a barostat balloon inflated in the stomach. Our finding that reduction of meal induced relaxation is not accompanied by an increase in perceived sensations questions the direct relationship between impaired accommodation and symptoms, as found in functional dyspepsia. Similar conclusions were drawn from a recent study showing that in patients with functional dyspepsia, abolishing gastric relaxation by the cholecystokinin A antagonist dexloxiglumide was associated with reduced rather than increased dyspeptic symptoms.32
In contrast with several animal studies, we did not observe an effect of l-NMMA on visceral perception. This may be explained by the knowledge that NO has been shown to be mainly involved in the perception of visceral pain.18,19,30,33 The healthy volunteers in our study predominantly reported bloating and satiation on gastric distension, rather than pain. One might however anticipate that NO synthase inhibition may have an effect on perception in dyspeptic patients with visceral hypersensitivity.6 Animal models of visceral hyperalgesia indeed show upregulation of NO synthase producing neurones in the spinal cord. More importantly, NO synthase blockade normalised the hyperalgesic response but had no effect on perception in control animals.33,34 Therefore, l-NMMA may only affect visceral perception in the presence of hypersensitivity. Further studies investigating the effect of NO synthase inhibition in patients with functional dyspepsia are therefore warranted.
The use of NO donors in conditions characterised by impaired accommodation and/or hypersensitivity to gastric distension is controversial. Nitrates are known to induce gastric relaxation and earlier studies showed some relief of symptoms in functional dyspepsia but not in diabetes.20,21 Moreover, significant side effects, in particular headaches, are associated with the use of nitrates. Therefore, development of fundus relaxing drugs may need to be aimed at selectively activating NO producing neurones at the level of the myenteric plexus. For example, the 5-HT1 agonist sumatriptan has been shown to relax the proximal stomach by activating NO producing neurones.11,35 Reduction of gastric tone by sumatriptan allowed higher gastric distension volumes in healthy volunteers before the threshold of discomfort was reached, and increased the amount of calories inducing maximum satiety in functional dyspeptics.1,7 Although these studies are promising, confirmation in larger clinical studies is awaited.
In summary, we showed that NO is involved in basal fundic tone and fundic relaxation in healthy volunteers but not in gastric perception. Reduction of meal induced relaxation did not result in increased perception of postprandial sensations. As NO inhibition did not affect gastric perception to distension and had no effect on sensations scored during intraduodenal lipid, the reduced scores for nausea and satiation by l-NMMA after oral meal intake are most likely caused by delayed gastric emptying.
Acknowledgments
SDK is supported by a grant from the Netherlands Digestive Diseases Foundation (MLDS), grant number WS 99-38. Parts of the study have been published previously in abstract form.