Article Text

Statistics from Altmetric.com
First described by Smith et al1 in 1982, Smith-Magenis syndrome (SMS) is a contiguous gene syndrome ascribed to interstitial deletions of chromosome 17p11.2. Clinical features include infantile hypotonia, characteristic craniofacial appearance, brachydactyly, short stature, ocular anomalies, deep, hoarse voice, early speech delay, mental retardation, and behavioural disturbances.2,3 Behavioural problems include hyperactivity, attention deficit, self-injury, temper tantrums, and major sleep disturbance.4 These symptoms have a major impact on the children and their families. The diagnosis is based on high resolution karyotype analysis and fluorescence in situ hybridisation (FISH).5
Sleep disturbances occur in all cases and are predictive of maladaptive behaviour, increased by mental retardation and cognitive delay. The specific pattern of sleep disturbance in SMS includes early sleep onset, frequent awakenings, and early waking.6,7 Moreover, “sleep attacks” at the end of the day are consistent features of the disease and may represent the endogenous sleep onset of the patients. The children could therefore be regarded as having a sleep phase advance.
Normally, melatonin secretion increases soon after onset of darkness, peaks at midnight, and gradually falls during the second half of the night. Interestingly, all SMS patients display a phase shift of their circadian rhythm of melatonin, with a diurnal secretion of the hormone8–10 (fig 1). Tantrums and tiredness occur when melatonin rises in the morning and children have naps and sleep attacks when melatonin peaks at midday and in the evening. Sleep is fragmented with prolonged nocturnal awakenings and early waking when melatonin is low during the night (fig 1). This clinical and biological sleep phase advance supports the existence of an aberrant biological clock in SMS.
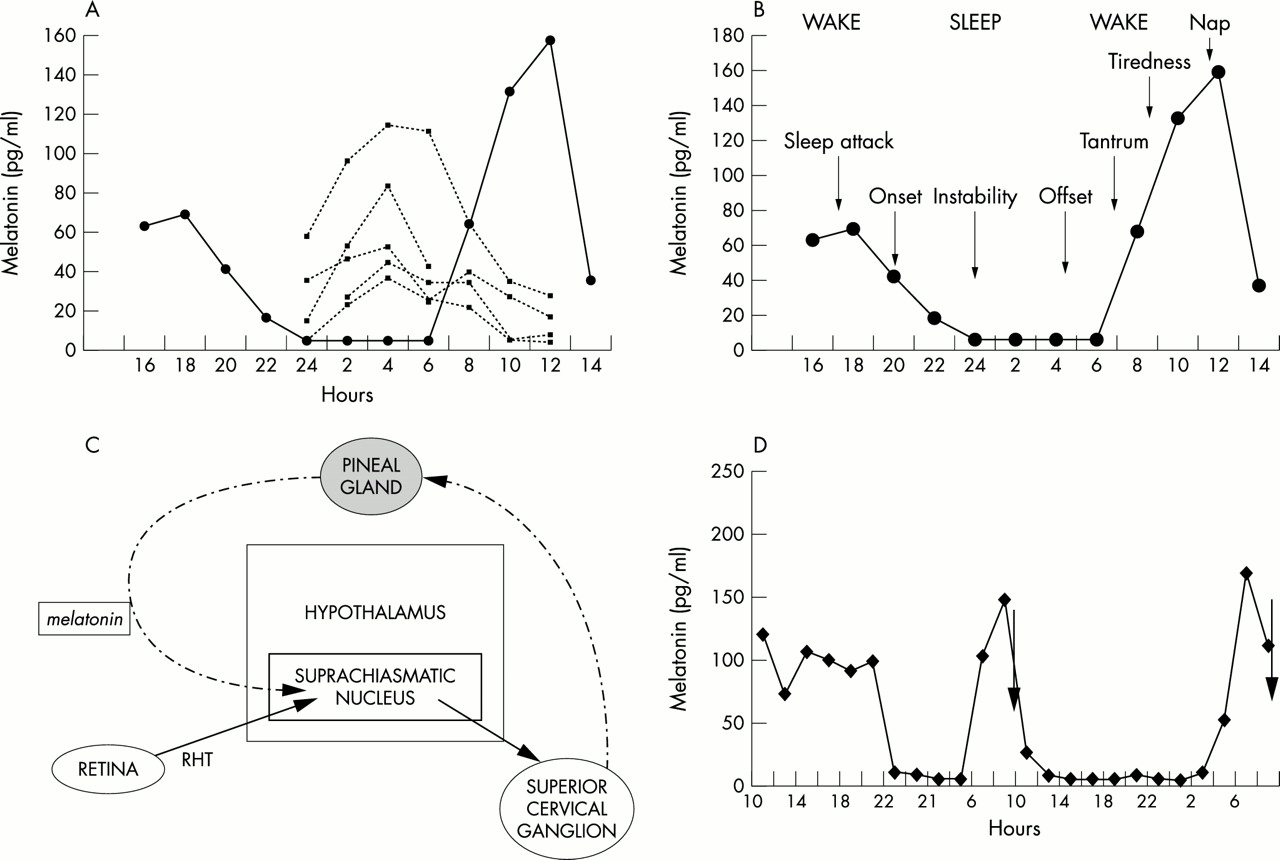
(A) Inversion of serum melatonin rhythm in SMS (solid lines) as compared to age matched controls (dotted lines). (B) Sleep-wake patterns correlated with melatonin secretion in SMS. (C) Melatonin secretion is under the control of photic information transmitted from the retina through the suprachiasmatic nuclei of the hypothalamus and sympathetic nervous system. (D) Circadian variations of plasma melatonin before and after β-adrenergic antagonist administration in SMS.
Because the circadian rhythm of melatonin is controlled by the sympathetic nervous system,11,12 SMS children were given acebutolol, as β1-adrenergic antagonists reduce the production of melatonin.13,14 Here, we show that the combination of morning β1-adrenergic antagonist and evening melatonin administration restored plasma circadian melatonin rhythm, decreased the frequency of behavioural disturbances, and enhanced sleep in SMS.
METHODS
Patients
Ten children (six boys, four girls, aged 4–18 years) were recruited from the cohort of SMS children diagnosed at Necker-Enfants Malades Hospital, Paris. The bioethical human research committee approved the investigation protocol and the parents signed an informed consent form before inclusion in the study. All SMS patients met the inclusion clinical criteria, namely: facial dysmorphism, developmental delay, speech delay, hyperactivity, attention deficit, and sleep disturbances. All carried a 17p11-2 deletion confirmed by FISH analysis using an ONCOR probe (D17S258). All 10 children underwent the first clinical trial comparing no medication to daytime β1-adrenergic antagonists to repress daytime melatonin.10 They were maintained on β1-adrenergic antagonist treatment during the time of the study. They did not receive other drugs in the course of the study.
Procedures
The patients’ sleep/wake schedules were investigated (1) before treatment, (2) on β1-adrenergic antagonist administration only, and (3) after two and six months of combined β1-adrenergic antagonist and melatonin administration. The consultations were performed by the same investigator (HDL). Sleep and day diaries were filled in at home by the parents over periods of one month for the duration of the 12 month study. For ambulatory actigraphy (nine patients), recordings were made during one minute periods, using the Actiwatch score (Cambridge Neurotechnology). Actiwatch is a lightweight, activity monitoring system worn on the wrist. Rhythmwatch software allows for a visual display of the activity-rest patterns and for the calculation of sleep-wake parameters over the entire length of the study. Outpatient actigraphy data were collected at home over a 21–28 day period during the month before and for the month after beginning melatonin administration. Actigraph data were analysed for average activity offset and onset, using the Actiwatch software programs.
Key points
-
Smith-Magenis syndrome (SMS) is a clinically recognisable contiguous gene syndrome caused by interstitial deletions of chromosome 17p11.2. The children have major sleep disturbances ascribed to a phase shift of their circadian rhythm of melatonin with a paradoxical diurnal secretion of the hormone.
-
Serum melatonin levels and day-night behaviour were studied in 10 SMS children (aged 4–18 years) given acebutolol, a selective β1-adrenergic antagonist (10 mg/kg early in the morning) and a slow release melatonin (6 mg in a single dose in the evening). Cardiac examination, serum melatonin, EEG, motor activity recordings, and sleep diaries were monitored before and after drug administration.
-
The present study shows that a morning dose of acebutolol and an evening dose of melatonin reset the biological clock and restore a normal circadian rhythm of melatonin in SMS. During the day, a significant improvement of inappropriate behaviour and an increased ability to concentrate were noted. During the night, delayed sleep onset, disappearance of night awakenings, increased hours of sleep, and delayed sleep offset were consistently observed.
-
These results suggest that β1-adrenergic antagonist and melatonin administration helps to manage hyperactivity, enhances cognitive performance, and reduces sleep disorders in SMS.
SMS children were given acebutolol, a selective β1-adrenergic antagonist (10 mg/kg at 8 am for six months). Starting on the evening of the first day of hospital admission, they also received an oral dose of a control release (CR) melatonin at 8 pm (same dose of 6 mg for all children tested). The treatment was pursued at home for up to six months, at the same dose, taken every morning at breakfast time and every evening half an hour before bed time.
The children were admitted for 48 hours to our paediatric unit for plasma melatonin and β-adrenergic metabolite monitoring between March and April 2001. Cardiac examination and ECG were conducted before drug administration and a 24 hour Medilog 9000 EEG recording (including six EEG channels, one ECG channel, one EMG channel) was conducted during hospitalisation. Blood samples were drawn from an indwelling forearm catheter every two hours, from 10 am on day 1 to 10 am on day 3 (two days, two nights). Samples were transferred to heparinised plastic tubes, centrifuged, and frozen at −20° until assay.
Melatonin was measured using a commercially available radioimmunoassay kit (melatonin direct RIA, IBL Hamburg). The minimal detection level of the test was 3.5 pg/ml. The intra-assay coefficients of variation for control samples were 8% and the corresponding interassay coefficients of variation were 14.9%. Previous studies have described the level of plasma melatonin in age matched controls.15 Levels of acebutolol and its active metabolite, diacetolol, were determined by a selective high performance liquid chromatography with fluorescence detection, excitation wavelength of 240 nm, and emission wavelength with a cut off filter of 418 nm. The coefficient of variation was in the range of 4.7–11.8% and the percentage of recovery was at least 96%.
Ethical reasons precluded including a control group of healthy children in this trial.
RESULTS
Monitoring endogenous plasma melatonin levels supported the blockade of melatonin secretion following β-adrenergic antagonist administration in SMS. Plasma acebutolol peaked 2.4 hours after the drug intake (plasma half life elimination was 7.4 ± 3.1 hours). The peak of diacetol (the main active metabolite of acebutolol) was reached approximately 3.5 hours after drug intake (plasma half life elimination 10.9 ± 4.7 hours). Consequently, mean melatonin levels remained low during the day and endogenous melatonin secretion was not restored by night. After a single CR melatonin administration, plasma melatonin levels rapidly increased in all SMS children (fig 2). Indeed, mean melatonin levels rose from 12.7 (SD 10.6) pg/ml to 2189 (SD 1800) pg/ml two hours after drug administration. Individual melatonin levels increased 170 fold, remained high from 10 pm to 2 am, and slowly decreased to 6 am.

Circadian variations of plasma melatonin in Smith-Magenis syndrome before (dotted line) and after β1-adrenergic antagonists alone (grey line) and after melatonin administration and β1-adrenergic antagonist administration (solid line). Blood samples were drawn every two hours over 48 hours in patients aged 15 years (A), 8–10 years (B-E), and 4 years (F). Acebutolol was given at 8 am and melatonin at 8 pm.
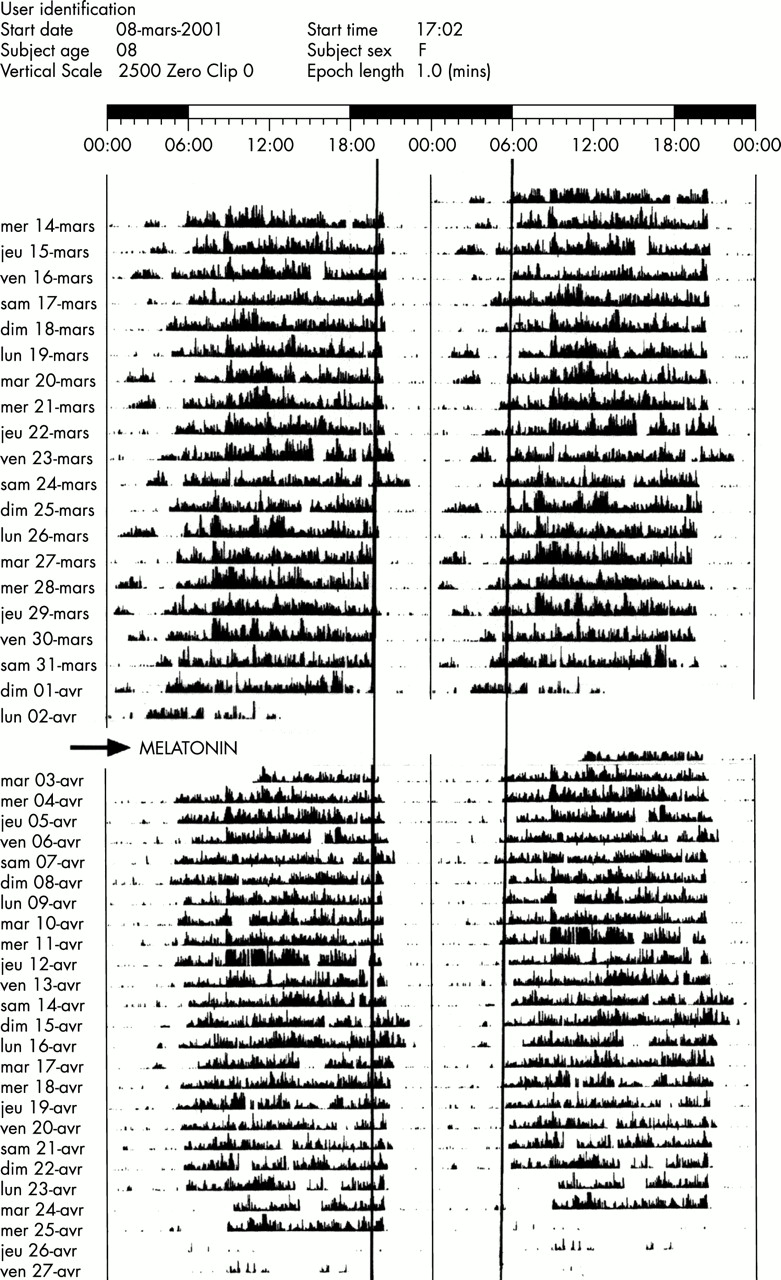
In one child (6 years), the treatment had to be discontinued after two weeks because he was unable to swallow the CR melatonin pills, but β1-adrenergic antagonist alone still improved family life. Giving CR melatonin markedly improved sleep disturbances in SMS. Indeed, before drug administration, mean sleep onset was 9.15 pm (range 8.30–10 pm), mean waking was 5.40 am (range 4–7 am), and mean duration of sleep was 8.20 hours (range 7.15–9 hours). Actigraphy data, collected over a 21–28 day period before and after melatonin administration, correlated with sleep and day diaries filled in at home by the parents. They showed that night parameters dramatically improved in children given both β-adrenergic antagonists and melatonin. In fact, based on actigraphy data, mean sleep onset was delayed to 9.45 pm (range 9–11 pm), mean waking to 6.40 am (range 6–8 am), and mean duration of sleep to 8.50 hours (range 8–9.30 hours) in SMS children given acebutolol and melatonin. Actigraphy data showed that the children did not wake up during the night (fig 3) and EEG recordings confirmed a more regular sleep stage organisation and a rapid access to sleep stage 3–4 (slow wave stage, not shown). Sleep was deep and quiet for both children and their family and day/night life was dramatically improved. Two children living in medical boarding schools were able share their room with other children, while they had to be locked in alone in their room before treatment. Two other children used to sleeping with their parents spent all night in their own bedroom. Parents no longer woke up by night in four other cases. However, sleep was not improved in one child (4 years). This child kept on waking up every night, but his mother was pregnant and gave birth to a baby by the time of the study. As treatment restored sleep in 8/10 cases, the children took a more active part in family and social activities during the day and had better adaptive behaviour in their institution. No desensitisation was observed over the six month period of drug administration. Finally, no side effects of β1-adrenergic antagonists or melatonin were noted and all parents asked for continuation of treatment at the end of the trial.

{kind=link}
{kind=link}
{kind=link}
Actigraphy of a 7 year old girl before and after melatonin administration. Recordings were made at one minute periods, using the Actiwatch score. Filled bars indicate periods of movement and activity.
DISCUSSION
SMS represents a model of sleep disturbance with a sleep phase advance and a phase shift of melatonin. We have hypothesised that sleep disturbances, behavioural problems, hyperactivity, and attention deficit could be related at least in part to inappropriate diurnal melatonin release (fig 1). Here, we show that β-adrenergic antagonist and melatonin administration reset the biological clock and improved sleep and behavioural disturbances in SMS. Indeed, β1-adrenergic antagonist lowered plasma melatonin levels, decreased motor hyperactivity, controlled outbursts, and reduced naps and sleep attacks during the day. Evening CR melatonin subsequently improved sleep patterns in all SMS children. Actigraphy data and sleep diaries showed a significant improvement of night parameters. Participation of the child in aspects of family life, which was hampered by fatigue and sleepiness, was markedly improved. After a single dose of exogenous melatonin, plasma melatonin levels rapidly peaked and slowly decreased, thus mimicking the effects of endogenous melatonin on circadian rhythm and sleep in SMS children. Mean sleep onset was delayed by 30 minutes, waking by 60 minutes, and the mean gain in sleep was 30 minutes. Waking inappropriately disappeared in most cases and wake up time was delayed. This study shows that CR melatonin is effective in sleep disturbance in SMS. No desensitisation was observed over six months. Because SMS is an infrequent disorder, we were unable to recruit a large enough group of age matched children to carry out a randomised double blind study.
Neurologically disabled and mentally retarded children also frequently exhibit disrupted sleep-wake cycles and severe sleep disturbances.16,17 The use of melatonin at the end of the day has been suggested for the treatment of chronic sleep disorders in disabled children.18–21 Since 1991, no adverse effect of melatonin use in disabled children has been noted.22 Melatonin, the main hormone of the pineal gland is synthesised from serotonin. Its synthesis and release are stimulated by darkness and inhibited by light. Photic information is transmitted from the retina to the pineal gland through the suprachiasmatic nuclei of the hypothalamus and the sympathetic nervous system.23 Normally, at twilight, the photoreceptors release norepinephrine, thereby enhancing the number of α1- and β1-adrenergic receptors in the pineal gland and activating N-acetyltransferase which triggers the synthesis and release of melatonin. For this reason, β1-adrenergic antagonists have been previously shown to reduce nocturnal plasma melatonin in young patients and to suppress inappropriate diurnal secretion in SMS.10
The abnormal circadian rhythm of melatonin in SMS and its relationship with chromosome 17 deletion remain unclear. It may result from an alteration of the input/output signalling pathway, for example, (1) photic entrainment in the retina/retinohypothalamic tract, (2) alteration of the circadian time keeping system (clock genes) of the suprachiasmatic nuclei, or (3) abnormal transmission from suprachiasmatic nuclei to an output signalling pathway of post-ganglionic fibres ascending to the pineal gland.24 Yet, how melatonin acts on sleep is at present unknown. It may modify brain levels of monoamine transmitters, thereby initiating a cascade of events culminating in the activation of sleep.25,26
In conclusion, this study suggests that elucidating pathophysiological mechanisms of behavioural phenotypes is particularly relevant to therapeutic approach in genetic diseases. Indeed, in SMS where the circadian rhythm of melatonin is shifted, our results indicate that β1-adrenergic antagonists combined with evening melatonin administration restored the circadian rhythm of melatonin, suppressed inappropriate diurnal melatonin secretion, and improved sleep and behavioural disorders.
Acknowledgments
We are grateful to the children, parents, and the ASM 17 family support group of France for participating in this study, and Pierre Frotte, M C Nolen, and Marie Noelle Rossillol for helpful cooperation. Part of this study was supported by Institut de Recherches Internationales Servier, Paris, France.