


Article Figures & Data
Figures
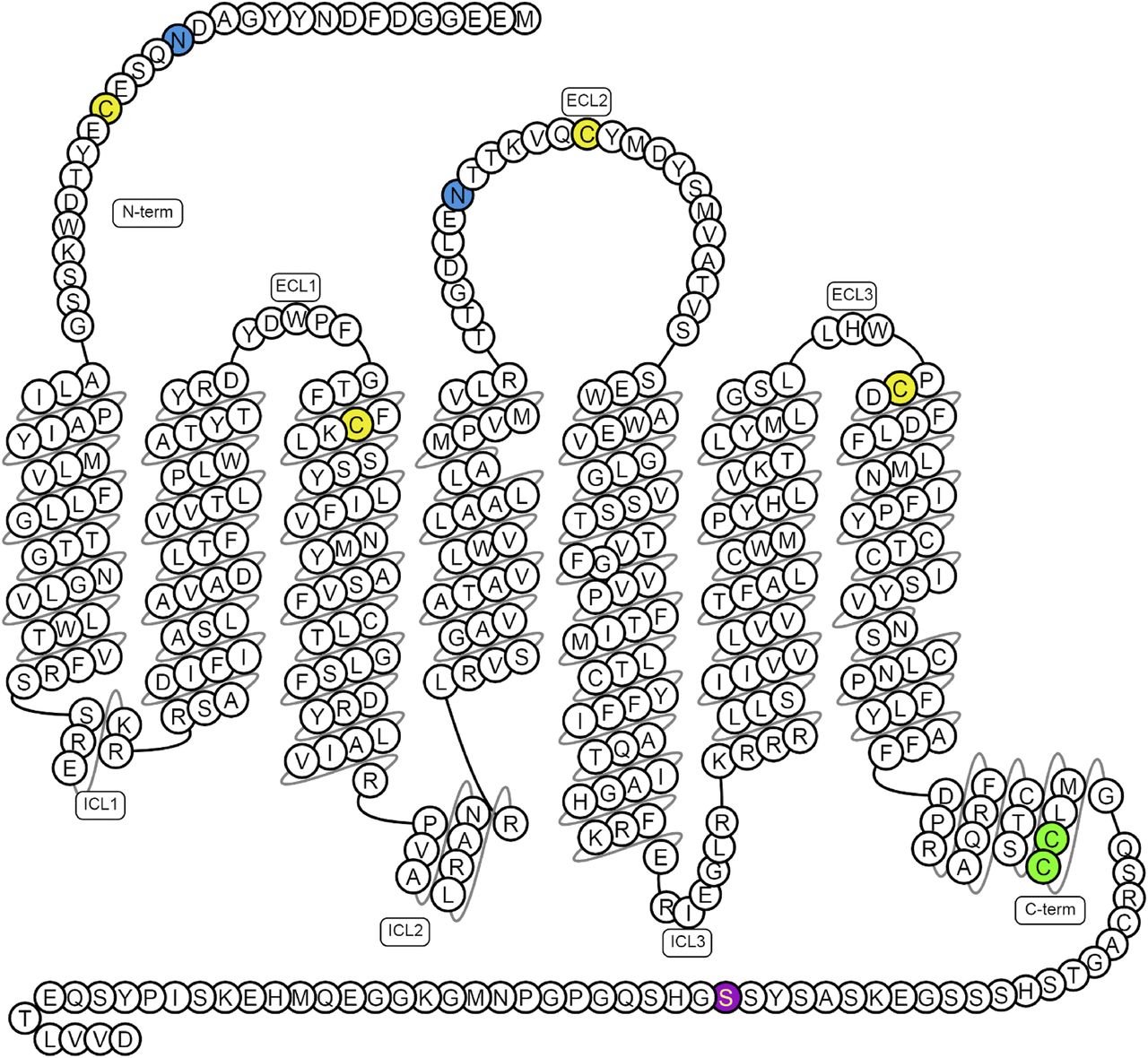
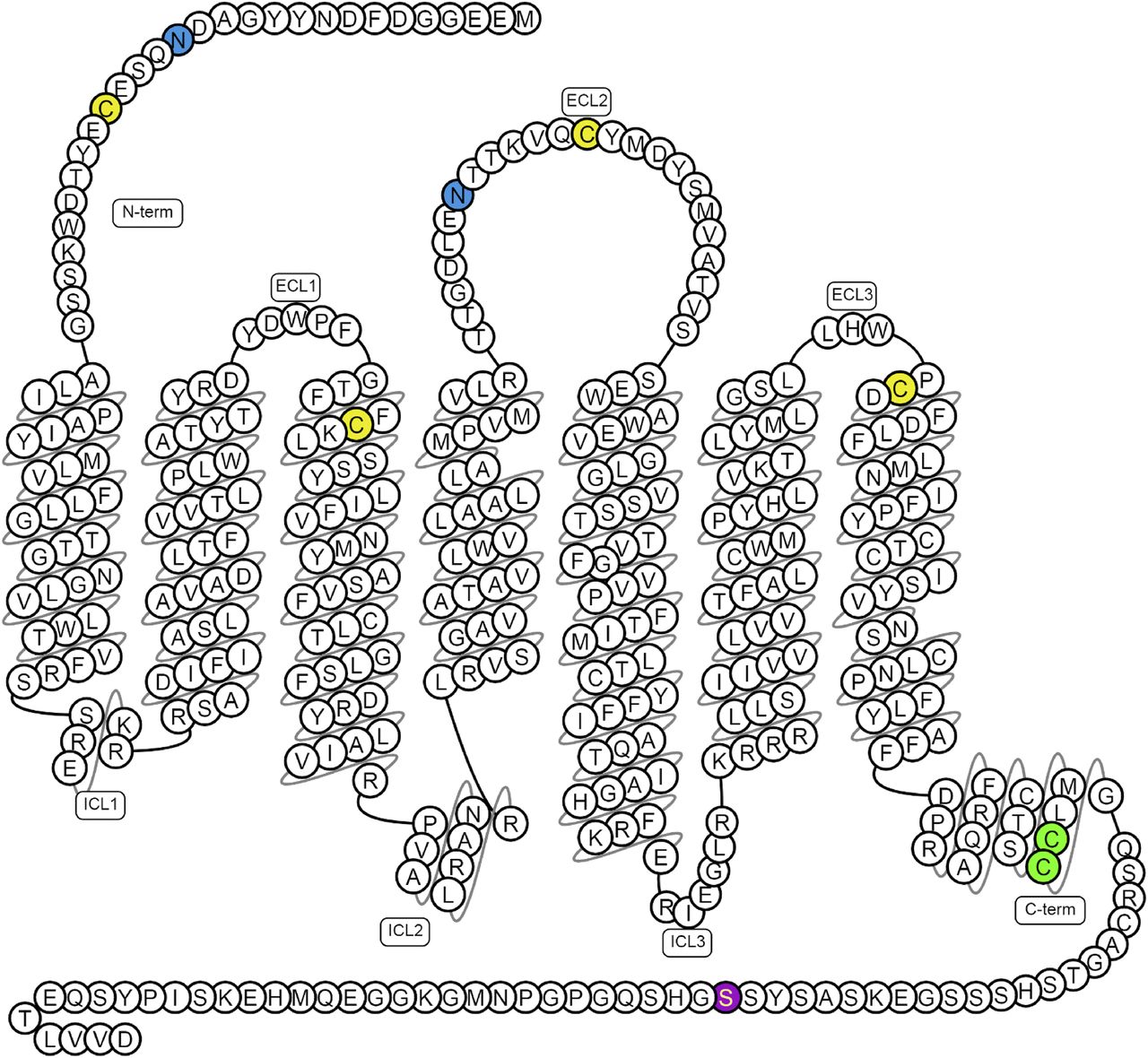
- Fig. 1.
Predicted disulfide bridges are between Cys19–Cys281 and Cys102–Cys181 (yellow); glycosylation sites (blue) are in the N-terminal tail (Asn15) and extracellular loop 2 (ECL2; Asn175); palmitoylation site (green) Cys325 and Cys326 and phosphorylation site (purple) Ser348 have been confirmed experimentally, of which Ser348 is crucial for apelin receptor interactions with GRK2/5, β-arrestin, and its internalization (Chen et al., 2014). Figure constructed from G protein-coupled receptor database (Pándy-Szekeres et al., 2018).
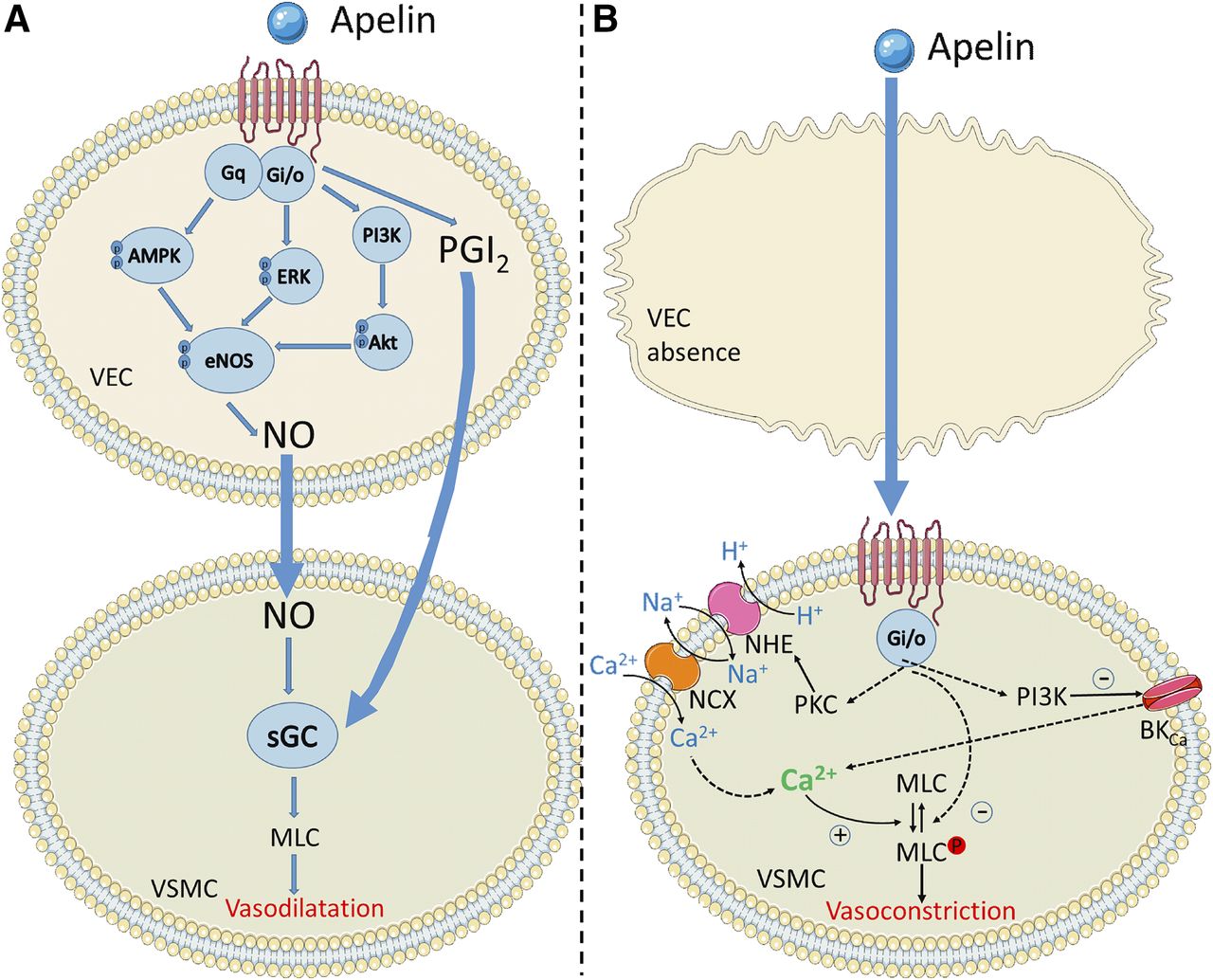
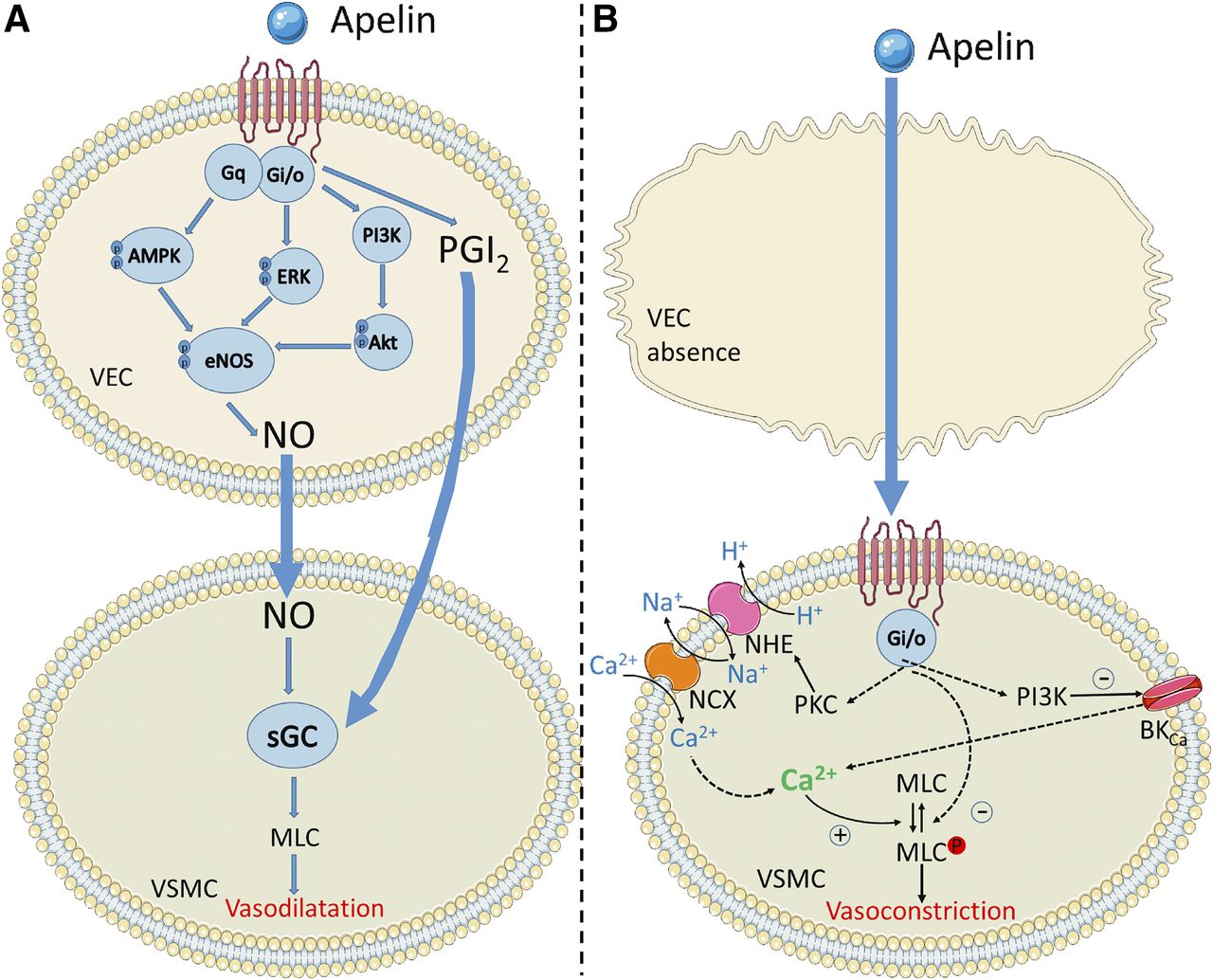
- Fig. 2.
The key signaling pathways suspected to be activated in vascular endothelial cells (VEC) and smooth muscle cells (VSMC) by the apelin receptor. Apelin binding can promote Gαi, Gαq, and β-arrestin recruitment to the receptor. In the presence of the endothelium, both Gαi and Gαq promote relaxation of smooth muscle cells through nitric oxide and prostacyclin release. In the absence of the endothelium, apelin binds directly to the receptor on the smooth muscle cells and leads to constriction through undetermined intermediate steps but most likely involving PKC, phosphoinositide 3-kinase (PI3K) and myosin light chain phosphorylation. Figure constructed using Servier Medical Art.
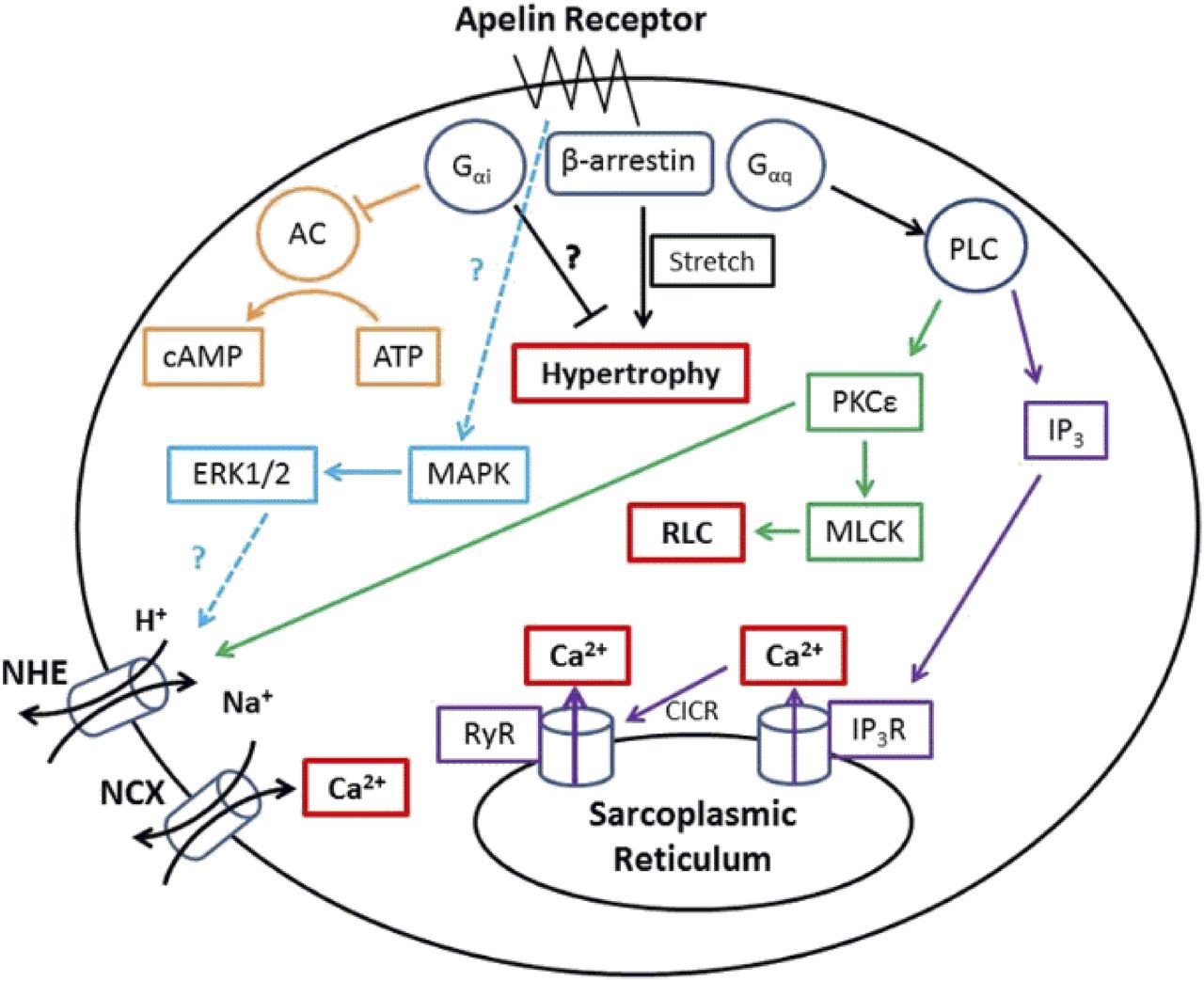
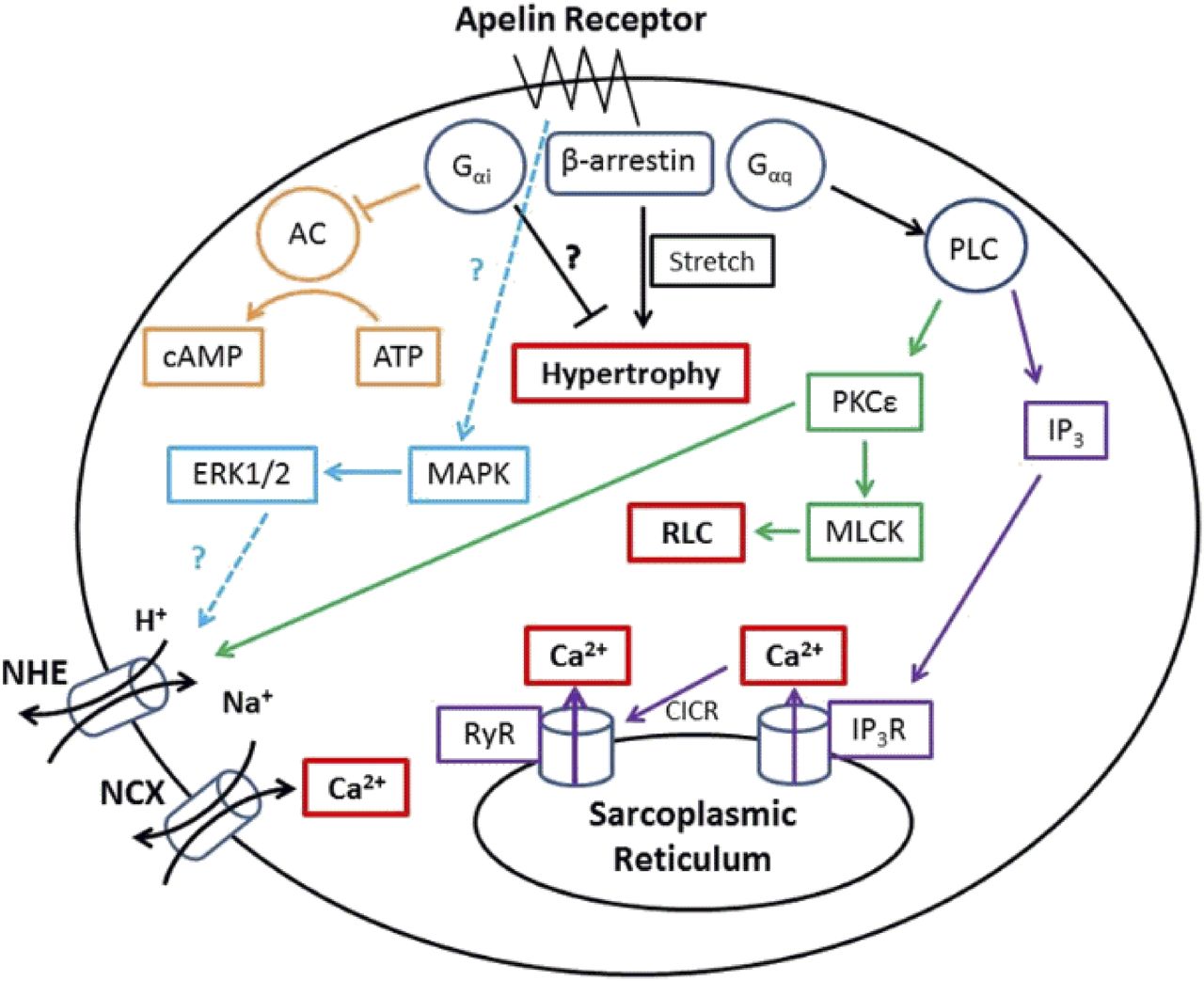
- Fig. 3.
The key signaling pathways suspected to be activated in cardiomyocytes by the apelin receptor. Apelin binding can promote Gαi, Gαq, and β-arrestin recruitment to the receptor, these pathways are thought to ultimately lead to cardiac inotropy without hypertrophy. However, in the absence of apelin, β-arrestin recruitment may lead to stretch-mediated hypertrophy.
- Fig. 4.
An overlay of ELA-11 (green) and apelin-13 (blue) docked in the apelin receptor binding pocket. The peptide sequences are shown alongside with the same color scheme. The red amino acids show where identical residues line up. Overlay from Yang et al., (2017b) under CC-BY license.
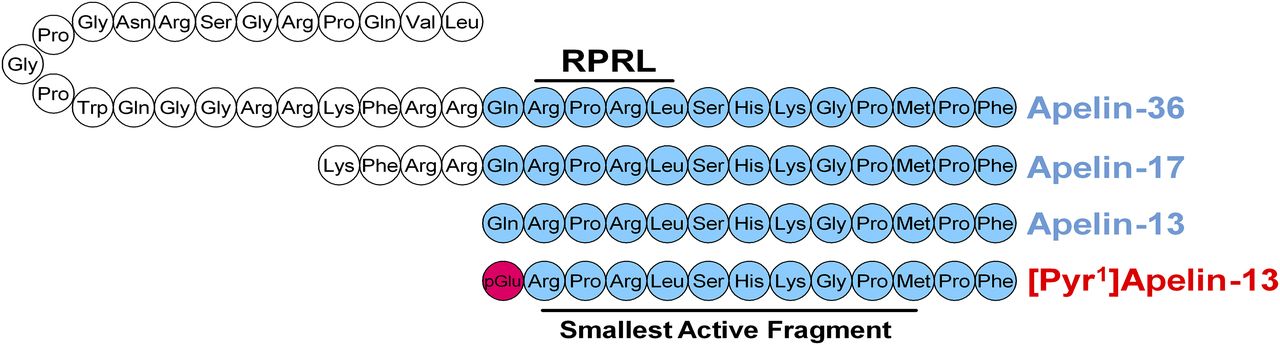
- Fig. 5.
The amino acid sequences of cleaved apelin fragments. [Pyr1]apelin-13 is the predominant form in the cardiovascular system and is shown in red with the pyroglutamate residue in pink. The smallest active fragment is highlighted, as well as the RPRL motif which has been thought critical to binding.
- Fig. 6.
The amino acid sequences of the predicted cleaved ELA fragments compared with [Pyr1]apelin-13, the predominant apelin isoform in the cardiovascular system. There is little sequence homology between ELA and apelin fragments; however, there are some similarities in the positioning of charged residues. Disulfide bridges are yellow lines, hydrophobic amino acids are shown in green, uncharged polar amino acids in pink, basic amino acids in blue and pyroglutamate in red. From Yang et al. (2017b) under CC-BY license.
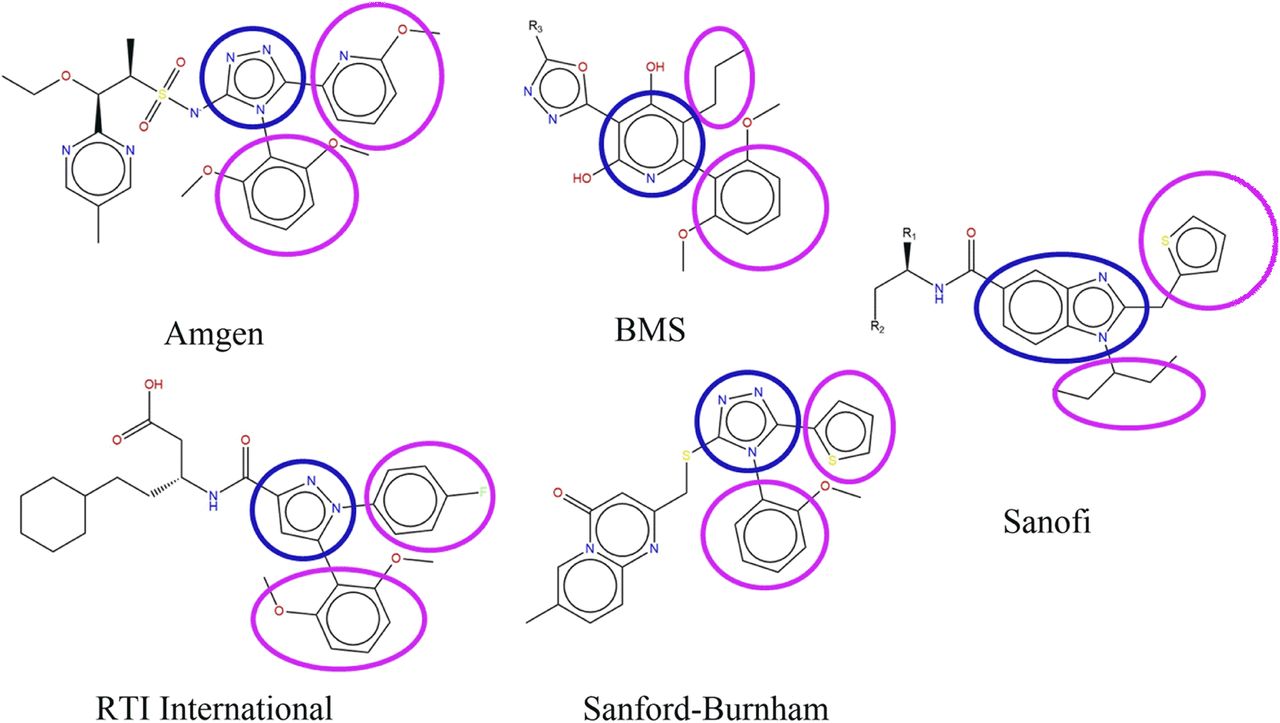
- Fig. 7.
The scaffold structures of five reported series of small molecule apelin agonists from Amgen (Chen et al., 2017), Bristol-Myers Squibb (Myers et al., 2017), RTI International (Narayanan et al., 2016), Sanford-Burnham (Pinkerton and Smith, 2015), and Sanofi (Hachtel et al., 2014). CMF-019 is derived from the Sanofi series. All of these molecules possess a broadly similar structure, consisting of two hydrophobic groups (circled in pink) extending from a heterocyclic core group (in blue).
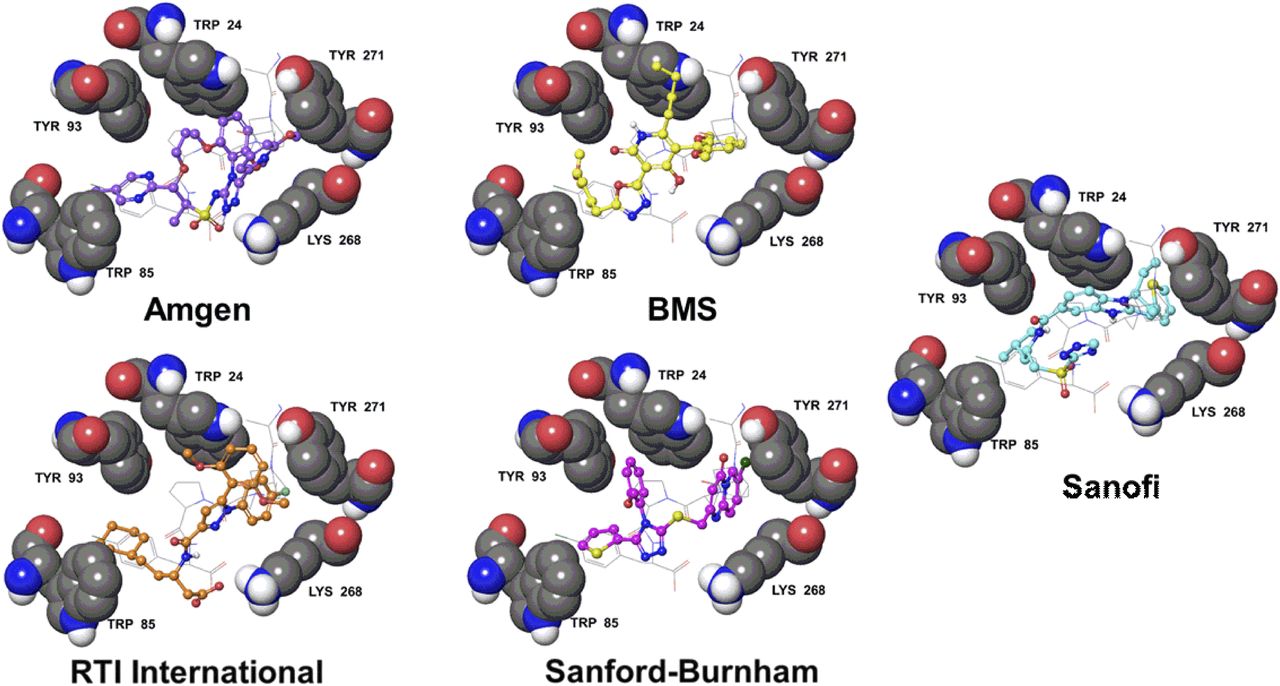
- Fig. 8.
The apelin receptor structure from PDBID 5VBL (Ma et al., 2017) with docked poses of five series of apelin agonists. The apelin receptor residues, W24, W85, Y93, K268, and Y271 are labeled and displayed as gray space filling. The structure of the four C-terminal residues of the apelin analog from PDBID 5VBL are displayed as gray sticks. The receptor and peptide are overlaid with docked poses of an Amgen (violet balls and sticks), a Bristol-Myers Squibb (yellow balls and sticks), an RTI International (orange balls and sticks), a Sanford-Burnham (magenta balls and sticks), and a Sanofi (cyan balls and sticks) small molecule apelin agonist. Only polar hydrogens are shown. Structures were derived from the following patents: Amgen (Chen et al., 2017), Bristol-Myers Squibb (Myers et al., 2017), RTI International (Narayanan et al., 2016), Sanford-Burnham (Pinkerton and Smith, 2015), and Sanofi (Hachtel et al., 2014). Pinkerton and Smith (2015) confirmed the Sanford-Burnham apelin compounds were selective vs. the angiotensin II receptor (AT1), the most closely related GPCR, with no significant off target binding.




Tables
- TABLE 1
Contacts between apelin-13 and the apelin receptor, inferred from the crystal structure PDBID 5VBL
Apelin-13 Contact Receptor Contacts References Q1 Sidechain D92a Gerbier et al., 2015 Q1 Backbone N177 P3 Sidechain T22 D23a Zhou et al., 2003a R4 Backbone D23a Zhou et al., 2003a L5 Sidechain E20a Zhou et al., 2003a T22 S6 Sidechain E174a Chapman et al., 2014; Gerbier et al., 2015 S6 Backbone Y21 H7 Sidechain E174a Chapman et al., 2014; Gerbier et al., 2015 K8 Sidechain Y21 Gerbier et al., 2015 D284a Ma et al., 2017 S275 G9 backbone Y271 P10 Sidechain E198a L173 Chapman et al., 2014 M11 Sidechain W24 Y271a Ma et al., 2017 F291 K268b Kumar et al., 2016 P12 Sidechain W24 Y93 P12 Backbone R168a Ma et al., 2017 F13 Sidechain W85a Y88 T89 Y93 Y299 F13 Carboxylate K268b Kumar et al., 2016 Y264 - TABLE 2
Expression of apelin receptor (APLNR), apelin, and ELA in mouse, rat, and human tissues
Compiled from Edinger et al. (1998), Hosoya et al. (2000), Lee et al. (2000), O’Carroll et al. (2000), Medhurst et al. (2003), Kleinz and Davenport (2005), Regard et al. (2008), Pope et al. (2012), Deng et al. (2015), Wang et al. (2015b).
APLNR Apelin ELA Human Rat Mouse Human Rat Mouse Human Rat Mouse Brain +++ ++ + ++ + +++ -paraventricular nucleus + ++ -supraoptic nucleus ++ ++ Anterior pituitary +a +++ +++ ++a +a Intermediate pituitary −/+ −/+ +/+++ Posterior pituitary −/+ −/++ +/++ Thymus + − + − Spinal cord + +++ ++ ++ ++ Cerebellum + + − + + − Hippocampus + + − + + Thalamus + + + + Heart + ++ +++ + ++ ++ −/+ + Adrenal gland + + + Lungs ++ +++ ++ + +++ ++ + Stomach + + + − + Liver + − + − − − Small intestine ++ + + − + Large intestine ++ + + + Pancreas + − + + Kidney + + + + + + ++ +++ Testis + + + + + ++ Prostate + + ++ Ovary + + ++ + + Uterus + + ++ − + − Placenta ++ ++ ++ Mammary gland + ++ Skeletal muscle + ++ ++ − + + Adipose tissue ++ ++ ++b ++ Cartilage ++ ++ Spleen +++ − + − + Skin + + Bladder + + Gall bladder + - TABLE 3
Some of the key agonists at the apelin receptor, their binding affinities, and whether they demonstrate bias compared with [Pyr1]apelin-13 (the predominant apelin isoform in the cardiovascular system (Maguire el al., 2009; Zhen et al., 2013) Endogenous agonists are denoted by “(E).”
Ligand Action Binding Affinity Units Bias References [Pyr1]Apelin-13 (E) Full Agonist 7.0–8.8 pIC50 — Kawamata et al., 2001 Medhurst et al., 2003 Apelin-13 (E) Full Agonist 8.8–9.5 pIC50 — Fan et al., 2003 Hosoya et al., 2000 Medhurst et al., 2003 Apelin-17 (E) Full Agonist 7.9–9.0 pIC50 β-arrestin El Messari et al., 2004 Medhurst et al., 2003 Apelin-36 (E) Full Agonist 8.2–8.6 pIC50 — Fan et al., 2003 Hosoya et al., 2000 Kawamata et al., 2001 Medhurst et al., 2003 Elabela/Toddler-11 (E) Full Agonist 7.2 pIC50 Yang et al., 2016 Elabela/Toddler-21 (E) Full Agonist 8.7 pIC50 β-arrestin Yang et al., 2016 Elabela/Toddler-32 (E) Full Agonist 8.7 pIC50 β-arrestin Yang et al., 2016 MM07 Full Agonist 9.5 pEC50 G protein Brame et al., 2015 CMF-019 Full Agonist 8.6 pIC50 G protein Read et al., 2016 ML233 Full Agonist — — — Khan et al., 2011 E339-3D6 Full Agonist 6.4 pKi — Iturrioz et al., 2010a - TABLE 4
Some of the key antagonists at the apelin receptor and their binding affinities
MM54, an antagonist at the β-arrestin and internalization pathway, consists of a cyclized peptide based around the RPRL motif. MM54 has been tested for selectivity (Bowes et al., 2012) against over 50 GPCRs (including the most closely related angiotensin II receptor AT1) and ion channels. ALX40-4C and protamine both consist of a series of positively charged amino acids and display low binding affinities and likely low selectivity for the apelin receptor.
Ligand Action Binding Affinity Units References MM54 Antagonist 8.2 pKi Macaluso et al., 2011 ALX40-4C Antagonist 5.5 pIC50 Zhou et al., 2003b ML221 Antagonist — — Maloney et al., 2012 Protamine Antagonist 6.4 pKi Le Gonidec et al., 2017 - TABLE 5
Some of the key radiolabeled ligands at the apelin receptor and their binding affinities
Ligand Action Binding Affinity Units References [125I][Nle75,Tyr77]apelin-36 (human) Full Agonist 11.2 pKd Kawamata et al., 2001 [125I][Glp65, Nle75, Tyr77]apelin-13 Full Agonist 10.7 pKd Hosoya et al., 2000 [125I][Pyr1]apelin-13 Full Agonist 9.5 pKd Katugampola et al., 2001 [3H][Pyr1][Met(0)11]-apelin-13 Full Agonist 8.6 pKd Medhurst et al., 2003 [125I]apelin-13 Full Agonist 9.2 pKd Fan et al., 2003 - TABLE 6
Apelin isoforms have comparable potencies at the apelin receptor expressed on cardiomyocytes, vascular endothelial and smooth muscle cells from human isolated cardiovascular tissue
EC50 values are geometric means. Values are mean ± S.E.M.
Action [Pyr1]Apelin-13 Apelin-13 Apelin-36 EC50 pD2 EMAX EC50 pD2 EMAX EC50 pD2 EMAX Inotropya 0.1 9.9 ± 0.2 49% 0.08 10.1 ± 0.3 64% 0.04 10.4 ± 0.2 39% Vasodilatationb 1.6 8.8 ± 0.1 39% 0.6 9.2 ± 0.2 51% 0.8 9.1 ± 0.2 43% Vasoconstrictionc 1.6 8.8 ± 0.5 30% 0.8 9.1 ± 0.2 19% 0.6 9.2 ± 0.5 17% EC50, the concentration (nmol/l) of apelin peptide producing 50% of the maximum response to that peptide; EMAX, maximum response, expressed as a % of a reference stimulus; pD2, negative log10 EC50.
↵a Human, electrically paced atrial strip. Maximum response is % inotropic response to calcium (8.95 mmol/l).
↵b Endothelium-dependent vasodilatation in human mammary artery pre-constricted with ET-1. Maximum response (EMAX) is % reversal of ET-1 response.
↵c Contraction of endothelium-denuded saphenous vein. Maximum response (EMAX) is %KCL (100 mmol/l). Tissues were maintained in organ baths at 37°C in oxygenated physiologic saline (Maguire et al., 2009).
- TABLE 7
Phenotypes observed in apelin, apelin receptor, and apela knockout mouse models
The lack of similarity between apelin and apelin receptor knock-out mice prompted the suggestion that there might be another ligand at the receptor. Apela knock-outs largely phenocopy the receptor knock-outs, supporting the idea that ELA is the missing endogenous ligand.
Apelin Knockout Mice Apelin Receptor Knockout Mice Apela Mutant Mice Mendelian birth ratio (Kidoya et al., 2008; Charo et al., 2009) Loss of homozygous mice (Ishida et al., 2004; Charo et al., 2009; Roberts et al., 2009; Scimia et al., 2012; Kang et al., 2013) Loss of homozygous mice (Freyer et al., 2017; Ho et al., 2017) Normal heart morphology (Kuba et al., 2007; Kidoya et al., 2008; Charo et al., 2009) Severe cardiac and vascular developmental defects (Kang et al., 2013) Severe cardiac and vascular developmental defects (Freyer et al., 2017; Ho et al., 2017) Normal blood pressure (Charo et al., 2009) Normal blood pressure (Ishida et al., 2004; Charo et al., 2009) Pre-eclampsia (Ho et al., 2017) Modest decrease in basal cardiac contractility (Charo et al., 2009) Modest decrease in basal cardiac contractility (Charo et al., 2009) ? Marked decrease in exercise capacity (Charo et al., 2009) Marked decrease in exercise capacity (Charo et al., 2009) ? Severe heart failure in response to pressure overload (Kuba et al., 2007) Markedly reduced heart failure in response to pressure overload (Scimia et al., 2012) ?
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- I. Introduction
- II. Recommendations for Nomenclature
- III. Apelin Receptor Structure
- IV. Apelin Receptor Signaling in the Cardiovascular System
- V. Endogenous Agonists
- VI. Apelin Receptor Distribution
- VII. Endogenous Peptide Distribution
- VIII. Synthetic Agonists
- IX. Synthetic Antagonists
- X. Radiolabeled Ligands
- XI. Apelin Physiology and Pathophysiology
- XII. Elabela/Toddler Physiology and Pathophysiology
- XIII. Human Polymorphisms
- XIV. Knockout Mouse Models
- XV. Conclusions and Perspectives
- Authorship Contributions
- Footnotes
- Abbreviations
- References
- Figures & Data
- Info & Metrics
- eLetters