Article Text

Abstract
Objective: Primary Sjögren syndrome (pSS) causes significant systemic symptoms including fatigue as well as glandular dysfunction. There are currently no effective systemic therapies; however, open label series have suggested that rituximab may be beneficial for systemic and glandular manifestations. Therefore, we performed a double blind, placebo-controlled, randomised pilot study of the efficacy of rituximab in reducing fatigue in pSS.
Methods: A total of 17 patients with pSS and a score on fatigue visual analogue scale (VAS) >50 were randomised to receive either 2 infusions of rituximab 1 g or placebo; patients also received oral and intravenous steroids. Outcome measures included: the proportion of patients with >20% reduction in fatigue VAS, changes in pSS related symptoms, health related quality of life and immunological parameters of pSS. These were measured 6 months after therapy.
Results: There was significant improvement from baseline in fatigue VAS in the rituximab group (p<0.001) in contrast to the placebo group (p = 0.147). There was a significant difference between the groups at 6 months in the social functioning score of SF-36 (p = 0.01) and a trend to significant difference in the mental health domain score of SF-36 (p = 0.06). There was one episode of serum sickness in the rituximab treated group.
Conclusions: This is the first double blind study of rituximab in pSS to show benefit; further studies are justified.
Statistics from Altmetric.com
Primary Sjögren syndrome (pSS) is a chronic autoimmune disorder affecting 0.2–3% of the population.1 Although the hallmark of the disorder is chronic inflammation of the salivary and lacrimal glands, systemic manifestations are common. Fatigue is prominent among these, has been found to be a major cause of disability for patients,2 and it is also regarded as a key symptom by doctors.3 The 36-item Short Form health questionnaire (SF-36) has identified substantially reduced health related quality of life in these patients and validated specific and sensitive tools have been designed to study fatigue in pSS.4
There is currently no proven effective systemic therapy for pSS. Neither corticosteroids nor disease modifying antirheumatic drugs (DMARDs) have been shown to have a significant effect on the disease course.5 6 Randomised, controlled studies have also failed to show significant differences between placebo and the anti-tumour necrosis factor (TNF) agents, infliximab and etanercept.7 8
The presence of autoantibodies, however, including anti-Ro, anti-La and rheumatoid factor (RF) as well as hyper γ-globulinaemia indicate a degree of B cell hyperactivity. Furthermore, B cell infiltrates, particularly of memory B cells, have been identified in salivary gland biopsy specimens.9
Recent open label studies have indicated efficacy of B cell depletion with rituximab, a chimaeric anti-CD20 monoclonal antibody first developed for the treatment of B cell lymphoma, a noted complication of pSS.10 Use of a variety of doses of rituximab, outcome measures (glandular and extraglandular) and timepoints11 12 led to the conclusion that randomised controlled trials were warranted in pSS. Furthermore, the efficacy of rituximab in rheumatoid arthritis13 and connective tissue diseases14 often associated with SS, suggests further clinical as well as theoretical grounds for use in pSS.
We therefore undertook an exploratory, pilot, randomised, double-blind, placebo controlled trial in order to determine the effect size of rituximab and thus whether a larger study would be feasible; this was in addition to assessment of the efficacy and safety of rituximab in pSS.
PATIENTS AND METHODS
This was a double-blind, randomised pilot study of rituximab vs placebo in 17 patients. The protocol was approved by the local ethics committees and all patients gave written, informed consent. Patients were enrolled at two sites in the UK.
Patients were eligible for the study if they fulfilled the American–European Consensus Criteria for pSS.1 Patients were required to be positive for either anti-Ro and/or anti-La antibody and to have scored >50 on a 100 mm fatigue visual analogue scale (VAS) (ranging from 0 for absence of fatigue to 100 for worst imaginable fatigue). Patients were excluded if they had active, concurrent depression or anxiety, other autoimmune disease or a history of solid organ malignancy.
Baseline evaluations included medical history, physical examination, routine haematology, biochemistry, hepatitis serology, electrocardiogram and chest radiograph. The following investigations were carried out to assess baseline disease activity: fatigue assessed by VAS and the Functional Assessment of Chronic Illness Therapy – Fatigue (FACIT-F) questionnaire;15 quality of life by SF-36 questionnaire;16 specific Sjögren related symptoms (for somatic fatigue, mental fatigue and sicca symptoms) by Profile of Fatigue and Discomfort (PROFAD) questionnaire3 (this is made up of domains scored individually; these scores can be added in various combinations eg, combined fatigue score (aggregate of somatic and mental fatigue), sicca score (aggregate of oral, ocular, skin and dryness) or combined fatigue and discomfort score (PROFAD = fatigue+arthralgia+vascular dysfunction)); Schirmer-1 test; unstimulated salivary flow rate test; erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). These investigations were repeated at monthly intervals after therapy for 6 months. RF and serum immunoglobulins were measured at baseline and 6 months.
Patients randomised to active therapy received two infusions of 1 g rituximab on days 1 and 15. Each infusion was preceded by 100 mg methylprednisolone, intravenously. Randomisation was performed by use of a computer-generated list, stratified by site. Following reports of serum sickness in patients with pSS treated with rituximab11 and after 1 serious adverse event in the second patient in this study (described below), 12 of the remaining patients received oral prednisolone between days 2–14, at a dose of 60 mg daily for days 2–7 and 30 mg on days 8–14. Patients could continue with concurrent medication but were prohibited from changing or adding disease modifying therapy during the course of the study. Patients were reviewed on a monthly basis for 6 months after therapy with a subsequent visit at 12 months after therapy for safety purposes.
This was a pilot study carried out to enable larger, controlled studies to be appropriately powered. The primary efficacy outcome was a 20% improvement in fatigue VAS score, 6 months after therapy. Secondary efficacy outcomes were derived from the measures of activity described above. Statistical analysis was carried out by t test for baseline data; χ2 test for primary outcome; t test for mean improvement in fatigue VAS and for laboratory outcomes (ESR, CRP, RF, serum Igs). Non-parametric statistical tests (Mann–Whitney U) were carried out for questionnaire derived outcome measures. As this was a pilot study, no formal power calculation in designing this trial was felt to be appropriate.
RESULTS
A total of 18 patients were recruited and full 6-month data are available for 17 subjects; 8 were randomised to receive rituximab and 9 received placebo. Baseline characteristics did not differ significantly between the two groups (table 1). Of note were high scores on fatigue VAS, 76 vs 69 mm and relatively long disease duration, 7.25 vs 8.25 years (for rituximab vs placebo). None of the patients had other significant systemic complications of pSS.
At 6 months, seven of eight patients receiving rituximab (87.5%) and five of nine patients receiving placebo (55.6%) demonstrated >20% improvement in fatigue VAS (χ2, p = 0.36) (fig 1). The mean improvement in fatigue VAS at 6 months was 49.5% (rituximab) vs 20.5% (placebo) (t test, p = 0.24). Using 30% improvement from baseline as a threshold for defining response, the number of rituximab responders was unchanged but fewer placebo patients (four of nine) achieved response (p = 0.064).

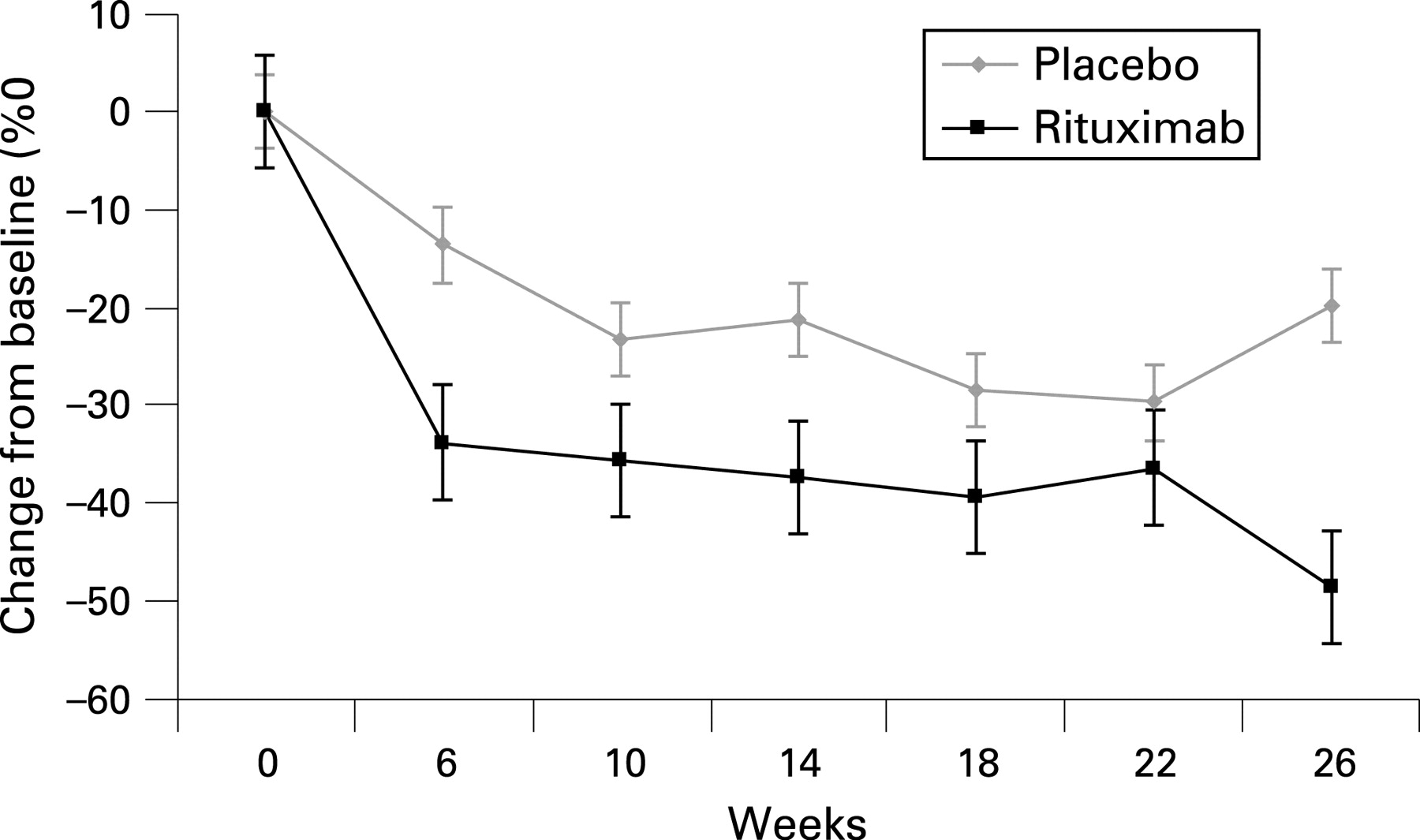
There was significant improvement from baseline in fatigue VAS in the rituximab group (mean (SD) improvement 36.8, (17.9), p<0.001) in contrast to the placebo group (mean improvement 17.3, (32.2), p = 0.147) (fig 2). General health VAS also improved significantly in the rituximab group (p = 0.021) but not in the placebo group (p = 0.96). Change in fatigue over time between the two groups indicated that the rituximab treated patients had greater reduction in fatigue than the placebo group at each month between treatment and 6 months afterwards (fig 3). The somatic fatigue domain of the PROFAD showed significant improvement in the rituximab treated group (p = 0.009) but not in the placebo group (p = 0.087). There was also a significant difference between baseline and 6 months in the rituximab treated group in PROFAD outcome (p = 0.026) but not in the placebo group (p = 0.219).

There was a significant difference at 6 months in the social functioning score of SF-36 (mean improvement in score, 12 vs −25, rituximab vs placebo, p = 0.01) and a trend to significant difference in the mental health domain score of SF-36 (mean improvement in score, 4 vs −24, rituximab vs placebo, p = 0.06). Patients treated with rituximab showed improvement in the mental component summary of the SF-3612 whereas patients who received placebo had deterioration (−8) (p = 0.06). No significant difference was observed in change in the physical health component of the SF-36 or in pain VAS.
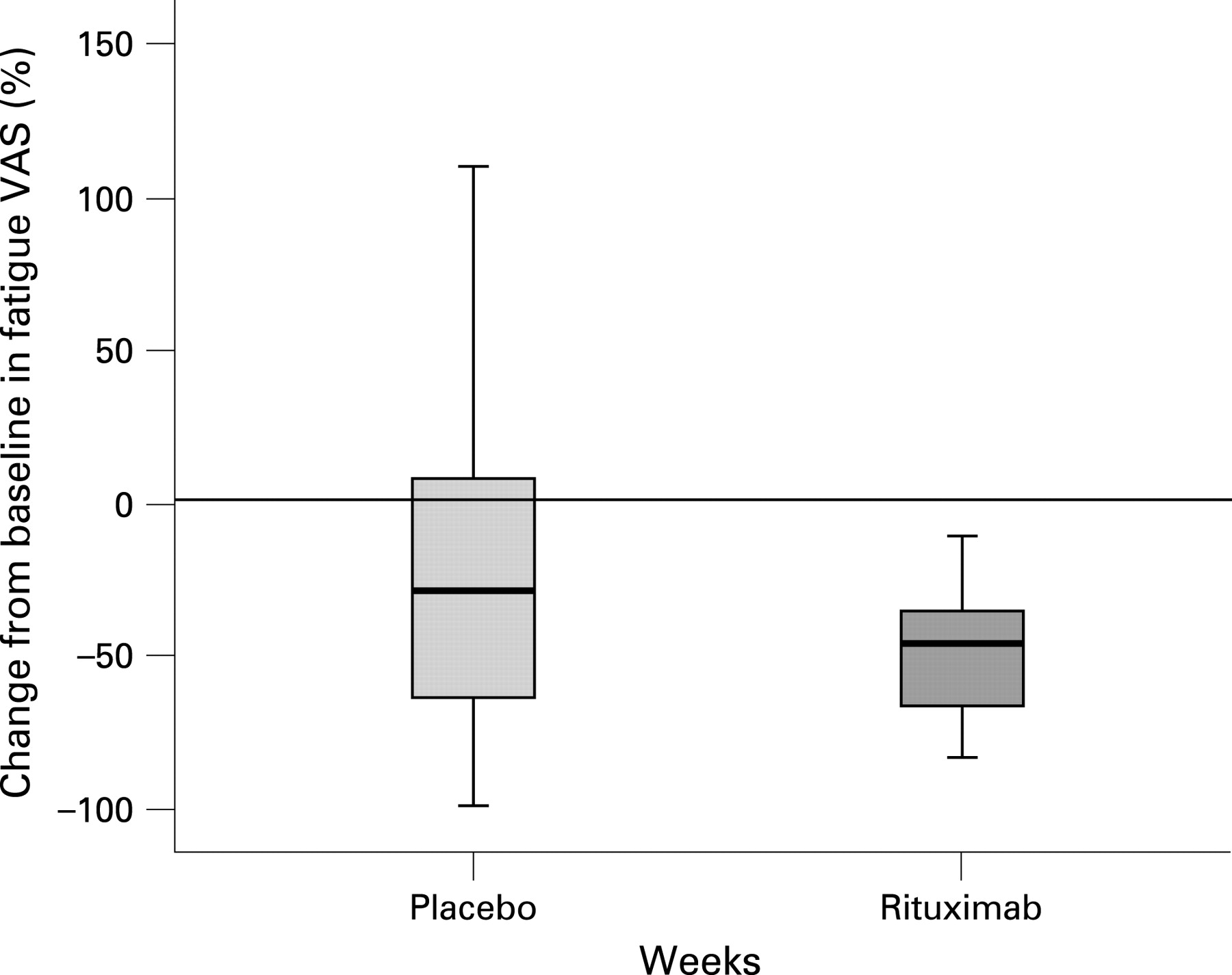
The change in fatigue VAS was much more variable in the placebo group (fig 4). In the placebo group, the change varied between approximately 99% improvement and 110% worsening (interquartile range 78%). In the active group the change varied between 83% improvement and 11% worsening (interquartile range 39%). In terms of laboratory outcomes, there was a significant difference in the reduction of RF between the two groups at 6 months (45 vs 0, rituximab vs placebo, p = 0.05) but no significant change was observed in immunoglobulin levels or titres or positivity for other antibodies. As only one patient in the active treatment arm did not respond, no specific analysis of whether baseline characteristics at baseline influenced outcome was undertaken. However, this non-responder did have less reduction in RF after treatment (16.7%) than the responders (mean reduction in RF 42.0% (21.8), range 17.4–67.9%)). This patient also had less reduction in immunoglobulin levels with 10.99% reduction in IgM, 2% reduction in IgG and 0.8% rise in IgA. Of the responders following rituximab, mean (SD) reduction in all immunoglobulins was noted: IgM 30.82% (21.99); IgG 12.42% (8.51); IgA 10.09% (13.11).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
No significant differences in glandular manifestations of pSS were observed at 6 months. There was no significant change in the Schirmer-1 test score or in unstimulated salivary flow rate at that timepoint. Following rituximab, seven of eight patients had B cell depletion <0.005×109/litre. At 6 months, B cell numbers were detectable above this level in seven of eight patients. There was no correlation between presence of B cells at 6 months and clinical status (at that timepoint).
Safety
Three serious adverse events (SAEs) occurred in two patients in the rituximab group. One patient developed symptoms of headache, urticarial rash, fever and meningism 7 days after the first infusion of rituximab. This was the second patient treated in the study and so she did not receive oral steroids as per the initial protocol. Infective meningitis was excluded and a diagnosis of serum sickness was made. The patient responded well to intravenous steroids. As a result of this episode, the study protocol was amended to include 2 weeks of oral steroid therapy (details above) between the two infusions of rituximab.
One other patient suffered two SAEs; the first was an admission to hospital for 24 h with abdominal pain, eventually diagnosed as gastroenteritis (4 weeks after the second infusion of rituximab) and this patient was also admitted to hospital for observation for palpitations for 24 h, 3 months after therapy. No significant cause for these symptoms was found.
Two patients in the rituximab group also experienced infusion reactions; these were both during the first infusion and consisted of rigors and a macular rash. The infusions were restarted and completed uneventfully after administration of antihistamine and hydrocortisone.
Pilot statistical analysis
Analysis of this pilot data indicates that a study with 37 patients in each arm would have adequate power to investigate the outcome used in this study ie, the hypothesis that rituximab therapy would lead to a 20% improvement in fatigue VAS score, 6 months after therapy over and above the improvement following placebo therapy.
DISCUSSION
This is the first randomised, double-blind, placebo controlled study of rituximab in treating fatigue in Sjögren syndrome. These results suggest that rituximab can improve fatigue in pSS. Rituximab also improved aspects of quality of life in pSS, with significant improvement in the social functioning domain score of SF-36 and a trend to significant improvement in the mental health domain score of SF-36. Rituximab therapy also significantly reduced RF levels over placebo without reducing overall Ig levels. This is the first therapy to show benefit over placebo in this disease and also indicates that fatigue is an important outcome measure that can be investigated usefully.
This study investigated improvement in fatigue as a primary outcome. Other studies of biological agents in pSS have used sicca symptoms or composite outcomes (sometimes including fatigue) as a primary outcome measure. The rationale for studying fatigue is that with pain it contributes more to quality of life than dryness.17 However, fatigue often has composite causes, including psychosocial. In this study, we attempted to minimise confounding factors for fatigue by excluding patients with active depression and anxiety and we screened for other disorders known to contribute to fatigue, such as thyroid disease.
This trial was designed as a pilot study. Patients receiving rituximab demonstrated greater mean improvement in fatigue although the results show a relatively high placebo effect for the 20% improvement threshold. It is calculated that a study with 37 patients in each arm would be adequately powered for this endpoint; by comparison, a pilot study of etanercept vs placebo in pSS8 calculated that an adequately powered study would require 288 subjects in total (albeit for different outcome, namely a composite of sicca symptoms and inflammatory marker/immunoglobulins). The “placebo” effect may be related to the role of steroids that were introduced following the occurrence of a serum sickness type reaction and reports of similar reactions in other studies. The dose of steroid used was identical to that in concurrent studies of rituximab in rheumatoid arthritis. In this study, patients treated with rituximab/steroids had greater reduction in fatigue than placebo/steroids only treated patients 1 month after therapy and this remained the case at each month thereafter. At 6 months, the effect of placebo/steroids was markedly variable, with striking improvement and deterioration. The improvement in the rituximab group was generally of a greater magnitude than in the placebo group and there was less variability supporting our hypothesis that rituximab has a beneficial effect on fatigue in pSS in patients who are positive for anti-Ro or anti-La autoantibodies. This greater improvement in the rituximab treated group was present immediately after treatment; at the week 6 timepoint, rituximab treated patients had 33% improvement in fatigue vs 15% in patients treated with steroid and placebo. This suggests that rituximab has a beneficial effect over and above that of oral prednisolone and the placebo group results at 6 months may simply be due to a true placebo effect. Limited longer-term data (at 12 months post therapy) is available (eight patients, four on rituximab, four placebo). These data indicate that responses to rituximab are sustained in some patients (58.7% improvement in fatigue VAS at 6 months vs 58.4% at 12 months) in contrast, patients receiving placebo had less improvement in fatigue VAS (35.5%) at 12 months.
Open label studies have suggested benefit in glandular manifestations of pSS but with increased disease duration, glandular atrophy rather than dysfunction is the major cause of dryness. In an open label series, those with lowest disease duration were more likely to show improvement in sicca symptoms after rituximab. Our patients had relatively long disease duration (7 vs 8 years, rituximab vs placebo) and thus change in sicca symptoms was perhaps less likely.
The safety profile of rituximab was generally satisfactory. No striking differences in the rates of infection or other adverse effects were seen between the two groups. Episodes of serum sickness have been reported previously only after the use of rituximab in Sjögren syndrome. The increased incidence of serum sickness in this group of patients is not entirely understood but it may be that the development and subsequent deposition of immune complexes is more likely because of hyper γ-globulinaemia in this population. The occurrence of infusion reactions and serum sickness may suggest that administration of rituximab with concomitant steroids should still be standard practice. Although rheumatoid factor fell, no reduction in overall immunoglobulin levels was seen, which is reassuring for safety, at least in the short term. This study also only enrolled patients who were positive for anti-Ro and/or anti-La antibodies; as this is in the light of data that rituximab was more effective in patients with RA positive for rheumatoid factor and/or anti-CCP antibodies, further studies of rituximab in pSS ought to focus on patients who are autoantibody positive.
The data from this pilot study suggest, therefore, that rituximab may well offer benefit for patients with Sjögren syndrome related fatigue and indicate that an adequately powered randomised study is feasible and justified.
Acknowledgments
We are grateful to our medical and nursing colleagues for their help with this project. We would also like to thank the patients who participated in this study. Elizabeth Hensor provided advice regarding statistical analysis.
REFERENCES
Footnotes
Funding: Roche UK provided study drug and an educational support grant to cover the costs of blood tests performed during this study.
Competing interests: None declared.
Ethics approval: The protocol was approved by the local ethics committees and all patients gave written, informed consent.