Article Text

Abstract
BACKGROUND More than 50% of patients with Parkinson’s disease develop motor response fluctuations (the “wearing off” phenomenon) after more than five years of levodopa therapy. Inhibition of catechol-O-methyltransferase by tolcapone has been shown to increase levodopa bioavailability and plasma elimination half life, thereby prolonging the efficacy of levodopa.
OBJECTIVES The primary objective was to evaluate the efficacy of tolcapone in reducing “wearing off” in levodopa treated, fluctuating parkinsonian patients. Secondary objectives included assessment of reduction in levodopa requirements, improvement in patients’ clinical status, duration of improvements, and tolerability of tolcapone.
METHODS In this multicentre, randomised, double blind, placebo controlled trial, 58 patients received placebo, 60 received 100 mg tolcapone three times daily (tid), and 59 received 200 mg tolcapone tid, in addition to levodopa/benserazide.
RESULTS After three months with 200 mg tolcapone tid, “off” time decreased by 26.2% of the baseline value, “on” time increased by 20.6% (P<0.01 v placebo), and the mean total daily levodopa dose decreased by 122 mg from the baseline dose of 676 mg (P<0.01). These responses were maintained up to nine months. With 100 mg tolcapone tid, “off” time decreased by 31.5% (P<0.05), “on” time increased by 21.3% (P<0.01), and the mean total daily levodopa dose decreased by 109 mg from the baseline dose of 668 mg (P<0.05). With 200 mg tolcapone tid, unified Parkinson’s disease rating scale motor and total scores were significantly reduced, and quality of life (sickness impact profile) scores were significantly improved. Both dosages were well tolerated. Dyskinesia was the most often reported levodopa induced adverse event. Diarrhoea was the most often reported non-dopaminergic adverse event and the most frequent reason for withdrawal from the study: four patients in the 100 mg tolcapone tid group and six in the 200 mg tid group withdrew because of diarrhoea.
CONCLUSION Tolcapone prolongs “on” time in fluctuating parkinsonian patients while allowing a reduction in daily levodopa dosage, thereby improving the efficacy of long term levodopa therapy.
- Parkinson’s disease
- tolcapone
- “wearing off” phenomenon
Statistics from Altmetric.com
Motor disability in Parkinson’s disease results primarily from the loss of dopaminergic input to the striatum.1 2 Parkinson’s disease affects one to two people in 1000 of the general population and 1% of people older than 65 years.3 The mainstay of treatment for Parkinson’s disease is levodopa (3,4-dihydroxy-L-phenylalanine), which is combined with a peripheral dopa decarboxylase inhibitor (benserazide or carbidopa) to prevent excessive peripheral levodopa metabolism.4
Although levodopa remains the single most effective antiparkinsonian drug available, more than half of all patients treated with levodopa for longer than five years experience complications such as dyskinesia and motor fluctuations, with progressively shortened periods of benefit from each dose, which in turn often necessitates more frequent levodopa doses.5 6
The mechanisms underlying this “wearing off” phenomenon are not fully understood but are at least partially connected with the peripheral pharmacokinetics of levodopa and its relatively short plasma elimination half life (about 1.5 hours).
Various pharmacological strategies have been used to smooth out these response fluctuations, including sustained release levodopa preparations, add on therapy with deprenyl or orally administered dopamine agonists, and subcutaneous apomorphine injections or infusions.7-11
Despite the addition of a peripheral decarboxylase inhibitor, levodopa is extensively metabolised in the periphery to 3-O-methyldopa (3-OMD) by catechol-O-methyltransferase (COMT).4 12 13 COMT thereby reduces the amount of levodopa available for conversion to dopamine. More speculatively, the resulting 3-OMD, which has an elimination half life of about 15 hours, accumulates in the plasma and can compete with levodopa for transport across the blood-brain barrier because these agents share a saturable carrier for membrane transport.14-16
Tolcapone (3,4-dihydroxy-4-methyl-5-nitrobenzophenone) is a potent, selective, reversible inhibitor of COMT.17 In animal studies, tolcapone has been shown to inhibit COMT activity in the gut, liver, and brain,18-20 and single oral doses of up to 800 mg were shown to be well tolerated in humans.6Pharmacological interaction studies of tolcapone and levodopa/decarboxylase inhibitor in healthy volunteers21showed that tolcapone roughly doubled the estimated area under the concentration-time curve and elimination half life of levodopa, whereas the average peak concentration remained unaffected. At the same time, the area under the curve for 3-OMD was reduced by up to 80%. By increasing the bioavailability of levodopa while maintaining more stable plasma concentrations, tolcapone could enhance the efficacy of levodopa therapy. Indeed, previous short term clinical studies have shown that the addition of tolcapone to levodopa therapy reduced “off” time and increased “on” time over a six week period in fluctuating parkinsonian patients.22 23
The primary aim of the present study was to assess the efficacy of tolcapone in reducing “wearing off” type motor fluctuations in parkinsonian patients receiving levodopa/benserazide therapy. Secondary objectives included evaluating the effect of tolcapone on levodopa requirements and the patients’ clinical status, the duration of these responses to tolcapone, and the tolerability of tolcapone when coadministered with levodopa/benserazide.
Materials and methods
STUDY DESIGN
This randomised, double blind, placebo controlled study was conducted at 24 centres in Europe and involved 177 patients from whom informed consent had been obtained. The trial was conducted in accordance with either the Declaration of Helsinki and its amendments or the laws and regulations of the country in which it was performed, whichever gave the patient greater protection.
Patients were screened for eligibility within the four weeks before randomisation. During this period, their antiparkinsonian therapy was stabilised. In addition, their ability to complete “on/off” self rating charts correctly (giving ratings for “on” and “off” time as a proportion of the waking day) was assessed because this evaluation method,24 which is now widely used in clinical trials, is essential in assessing the impact of treatment. Furthermore, in a previous study,25 data from patient diaries showed good correlation with data from investigators’ assessments of actual motor performance. Patients were given examples and instructions on how to complete the self rating charts and had to complete accurately six charts on any three typical days during each of the two weeks before baseline to be eligible for inclusion in the study. If more than six charts were completed, only the last three from each week were used for analysis to minimise bias.
Eligible patients were randomised to receive either placebo or 100 or 200 mg tolcapone three times daily (tid) The study had a common closing date design and was planned to end when all patients had received test medication for three months (the primary end point) and at least 30% had completed a 12 month assessment. However, only 15% reached the 12 month assessment because of the common closing date, so a secondary end point of nine months was selected instead for maintenance of response analyses of the 38% of patients who reached this time point.
PATIENTS
Patients of either sex with at least two of the three cardinal features of Parkinson’s disease (bradykinesia, resting tremor, and rigidity) and who exhibited predictable end of dose motor fluctuations in response to levodopa therapy were recruited to the study.
Eligible patients were at least 30 years old at the onset of symptoms, had been treated with levodopa for at least one year, had shown clear improvement in the clinical features of Parkinson’s disease with this treatment, and had been on a stable regimen of levodopa/benserazide and any other antiparkinsonian drugs for at least four weeks. Women were either postmenopausal or using a reliable method of contraception.
Patients with non-idiopathic parkinsonism (for example, progressive supranuclear palsy, striatonigral degeneration, or sporadic olivopontocerebellar atrophy) were excluded, as were patients who exhibited sudden, unpredictable “on/off” fluctuations or diphasic dyskinesia. Those who had a mini mental state examination score of 25 or less, who had had a major depressive episode in the preceding six months, or had a psychiatric or medical condition that might place them at increased risk or interfere with assessment of Parkinson’s disease, or who had undergone neurosurgery during the previous year were excluded. Treatment with any of the following medications also resulted in exclusion from the present study: a centrally acting dopamine antagonist during the preceding six months (the peripherally acting dopamine antagonist domperidone was permitted), a monoamine oxidase inhibitor (except selegiline) in the preceding two months, apomorphine in the preceding seven days, or any investigational agent within the preceding four weeks (or within five half lives of the compound, whichever was longer).
TREATMENT
Tolcapone dosages of 100 and 200 mg tid (administered orally) were selected on the basis of pharmacokinetic results from multiple dose studies in healthy volunteers,6 26 which indicated that the clinical effect of tolcapone shows a plateau at these dosages. Riboflavin (0.5 mg) was included in the placebo tablets to mimic the yellow discoloration in urine that occurs with tolcapone as a harmless side effect. The first daily dose of tolcapone or placebo was taken with the first dose of levodopa; the remaining two doses were taken at six hourly intervals thereafter.
After the first day of study treatment, the levodopa dosage could be adjusted as necessary, according to patient response and the development of adverse effects. However, levodopa adjustment was not permitted during the two weeks preceding the three month assessment, so that the efficacy of tolcapone could be assessed under a stable levodopa regimen at the primary end point. Increases in daily levodopa dosage above the baseline level were not permitted before month 3.
STUDY ASSESSMENTS
The efficacy and tolerability of tolcapone were assessed at the clinic between weeks 1 and 2 and at the end of week 6 and months 3, 6, 9, and 12.
The primary efficacy index was the change in proportion of “on” and “off” time between baseline and month 3; this was measured using self rating charts, which the patients completed during a 16 hour period on any three typical days during the week before each clinic visit. Patients were required to provide ratings each hour for the two preceding 30 minute periods. A carer was allowed to assist the patient in marking the diary, but the patient had to decide on the ratings. Mobility was rated as “on” (good or practically normal mobility), “intermediate” (neither “on” nor “off”), or “off” (stiffness, decrease in mobility or immobility). The individual values for “on”, “intermediate”, and “off” periods were calculated as a percentage of a standardised 16 hour waking day.
For the secondary indices, investigator’s global assessments (IGAs) were used to evaluate the degree of change between pretreatment and post-treatment—that is, the overall efficacy of tolcapone, compared with placebo, at the primary end point. The investigators used nine point scales to describe the severity of parkinsonian symptoms, the “wearing off” phenomenon, overall efficacy, and overall tolerance, ranging from 4 (very marked improvement) to −4 (very marked deterioration), and a seven point scale to evaluate dyskinesia, from 3 (marked reduction) to −3 (marked increase).
The unified Parkinson’s disease rating scale (UPDRS) was used to provide quantitative and qualitative measures of the severity of Parkinson’s disease. At screening, baseline, and subsequent clinical visits, scores from UPDRS subscales I (mentation, behaviour, and mood), II (activities of daily living during “on” and “off” periods), and III (motor function during “on” periods) were assessed.
The sickness impact profile (SIP) was completed by patients at baseline and at the three and 12 month visits and was used to evaluate patients’ quality of life. The SIP27 comprises 136 items considering 12 distinct domains of quality of life: ambulation, mobility, body care, social interaction, communication, alertness, emotions, sleep, eating, work, household management, and recreation. In addition to scores for each of the 12 domains, summary scores were calculated for physical, psychosocial, and total behavioural dysfunction. Details of total daily levodopa dosage were recorded at all assessment visits.
Adverse events were evaluated by spontaneous reports and observation of patients at assessment visits. Patients were also asked to rate the intensity of 13 levodopa induced symptoms (including gastrointestinal, neurological, cardiovascular, and psychiatric disorders) if these had occurred during the four days before the visit. Levodopa induced dyskinesia was assessed using UPDRS subscale IVa and a five point dyskinesia rating scale, ranging from 0 (no dyskinesia) to 4 (violent dyskinesia, incompatible with normal motor tasks).
Vital signs (supine and standing pulse rate and blood pressure), a 12 lead ECG, and laboratory variables were recorded at clinic visits throughout the study and data were screened for values outside the predetermined normal ranges.
STATISTICAL ANALYSES
Efficacy and tolerability analyses were performed on all patients who had been randomised to treatment, who had taken at least one dose of study medication, and who were subsequently seen at least once (the intention to treat population). The Bonferroni-Holm procedure was applied for pairwise comparisons of effficacy between placebo and each dosage of tolcapone to adjust for multiple comparisons. The continuous variables (“on/off” time, UPDRS total, and subtotal scores for subscales I to III, SIP scores, total daily levodopa dose, and number of daily levodopa doses) were analysed using two way analysis of covariance (ANCOVA) techniques.
For each treatment, we report least squares estimates of the mean treatment effects—that is, unweighted averages of centre means with the covariate at its mean value. The categorical variables (IGAs) were analysed by the Cochran-Mantel-Haenszel test, using centre as a stratification factor. The Breslow-Day test for homogeneity was applied for paired comparisons to test for consistency of response outcome across centres.
Results
After randomisation, 58 patients received placebo, 60 received 100 mg tolcapone tid, and 59 received 200 mg tolcapone tid. Table 1 shows the baseline demographic data, key Parkinson’s disease characteristics, and levodopa dosage.
Baseline demographic data and key characteristics of Parkinson’s disease
EFFICACY
Primary measures at three month end point
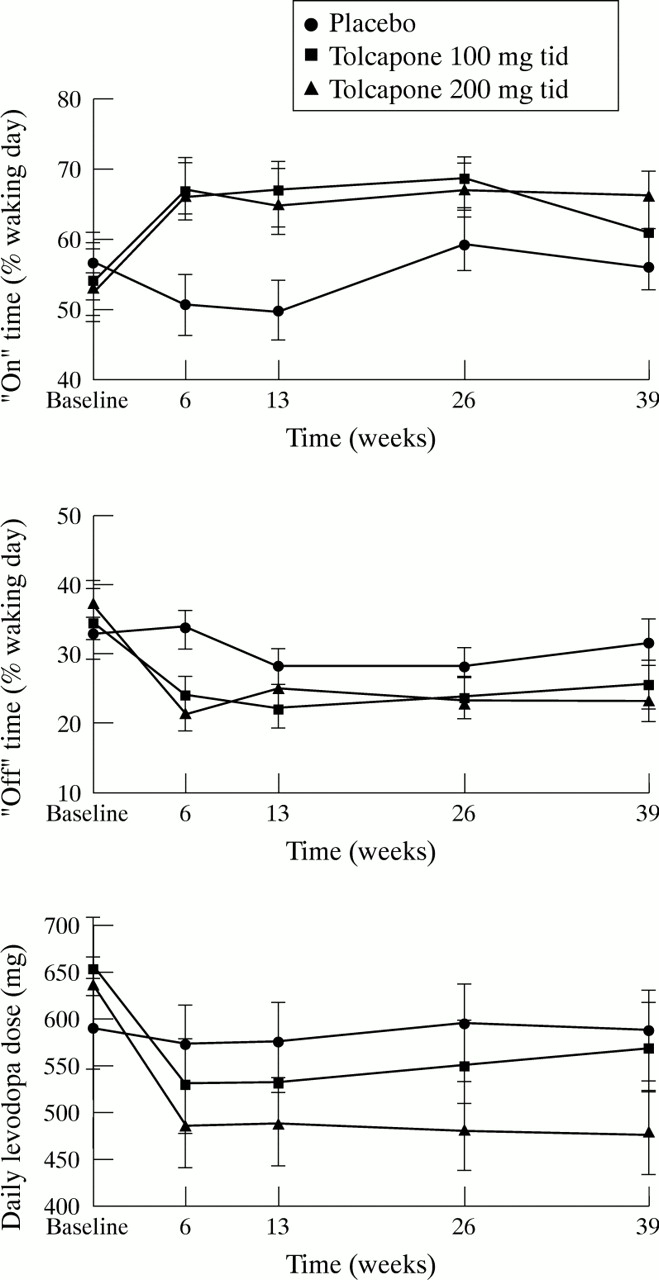
With 100 mg tolcapone tid, “on” time increased by 21.3% of the baseline value (P<0.01 v placebo) and “off” time decreased by 31.5% (P<0.05). With 200 mg tolcapone tid, “on” time increased by 20.6% (P<0.01) and “off” time decreased by 26.2% of the baseline value (non-significant). Table 2 and figure 1 summarise the efficacy data showing alleviation of the “wearing off” phenomenon and the change in daily levodopa dosage at the primary end point.
Efficacy data assessed by changes in “on/off” time and total daily levodopa dose and by IGAs of efficacy at the primary endpoint

Efficacy results at month 3, assessed by changes in (A) “on“ time, (B) “off” time, and (C) daily levodopa dose. Data are least squares means (SEM). “On” time and “off” time are presented as a percentage of the 16 hour waking day. *P < 0.05; **P < 0.01 v placebo.
Secondary measures at three month end point
The least squares mean (SD) reductions in total daily levodopa dose were 108.9 (23.4) mg (P<0.05) in the 100 mg tolcapone tid group and 122.2 (23.9) mg (P<0.01) in the 200 mg tid group. Both decreases were significantly different from the 28.9 (26.2) mg levodopa reduction found with placebo.
Scores on UPDRS subscales I (mentation) and II (activities of daily living) did not change significantly between baseline and month 3 in each of the three groups. The score for UPDRS subscale III (motor function) was reduced by 2.1 (1.1) in the placebo group, 4.2 (1.0) in the 100 mg tolcapone tid group (not significant), and 6.5 (1.0) in the 200 mg tid group (P<0.01).
Least squares mean reductions in SIP total, physical, and psychosocial scores between baseline and month 3 were greater with tolcapone than with placebo, indicating an improvement in quality of life with tolcapone during this period. Total SIP scores were reduced by 0.9 (0.9) in the placebo group, 1.9 (0.9) in the 100 mg tolcapone tid group, and 4.2 (0.8) in the 200 mg tid group (P<0.05). Physical scores were reduced by 2.2 (1.2) with placebo, 3.2 (1.1) with 100 mg tolcapone tid, and 5.0 (1.1) with 200 mg tid. Psychosocial scores were reduced by 1.2 (1.3) with placebo, 1.3 (1.2) with 100 mg tolcapone tid, and 4.7 (1.2) with 200 mg tid (P<0.01).
Table 2 shows the IGAs of efficacy. The IGA of overall efficacy of parkinsonian treatment showed that, by month 3, significant changes from baseline occurred in both tolcapone groups compared with placebo (P<0.01). Overall efficacy was improved in 70% of patients in the 100 mg tolcapone tid group and in 78% in the 200 mg tid group, compared with only 37% in the placebo group. The incidence of “very marked improvement” was found to be greatest with 200 mg tolcapone tid
Secondary measures until nine month end point
We originally planned to evaluate maintenance of response at the last time point at which at least 30% of patients were still receiving treatment—that is, 12 months. However, because the common closing date of the study resulted in more patients receiving study treatment for nine months (29% of the placebo group, 39% of the 100 mg tolcapone tid group, 46% of the 200 mg tid group) than for 12 months (14% of the placebo group, 17% of the 100 mg tolcapone tid group, 15% of the tolcapone 200 mg tid group) we selected a secondary time point of nine months, thereby maintaining our originally planned sample size.
Figure 2 shows the results of these maintenance of response analyses.

Maintenance of response up to month 9, assessed by changes in (A) “on” time, (B) “off” time, and (C) total daily levodopa dose. “On” time and “off” time are presented as a percentage of the 16 hour waking day. Data are means (SEM).
With 200 mg tolcapone tid, the increase in “on” time, decrease in “off” time, and reduction in levodopa dosage found at month 3 were maintained until month 9.
With 100 mg tolcapone tid, only the decrease in “off” time was maintained until month 9.
TOLERABILITY
Both tolcapone dosages were generally well tolerated. Table 3shows the adverse events that were reported at least 5% more often by patients receiving tolcapone than by those receiving placebo. Many of these (dyskinesia, nausea, vomiting, insomnia, orthostatic complaints, muscle cramps, excessive dreaming, and somnolence) are known to occur with levodopa therapy in patients with fluctuating Parkinson’s disease. The principal non-dopaminergic events reported were diarrhoea, headache, and abdominal pain.
Adverse events reported by patients on tolcapone with incidences >5% higher than reported by patients on placebo
Twenty seven patients withdrew prematurely from the study because of adverse events: four (7%) from the placebo group, 14 (23%) from the 100 mg tolcapone tid group, and nine (15%) from the 200 mg tid group. Of the adverse events leading to withdrawal, only diarrhoea had a higher incidence with tolcapone than with placebo. No patients in the placebo group withdrew because of diarrhoea, compared with four (7%) in the 100 mg tolcapone tid group and six (10%) in the 200 mg tid group. These withdrawal rates were similar to the number of reports of severe diarrhoea: none in the placebo group, three of nine cases with 100 mg tolcapone tid, and six of 15 cases with 200 mg tid Although dyskinesia was the most often reported levodopa induced adverse event from the start of the study, it resulted in the withdrawal of only two patients (one from each tolcapone treatment group). Hallucinations led to the withdrawal of two patients in the 100 mg tolcapone tid group and one patient in the 200 mg tid group. Orthostatic hypotension led to the withdrawal of only one patient overall (from the 100 mg tolcapone tid group).
Most patients exhibited levodopa induced dyskinesia at baseline: 57% in the placebo group, 66% in the 100 mg tolcapone tid group, and 69% in the 200 mg tid group, according to the dyskinesia rating scale. No significant changes in incidence from baseline were found in any group during the study. The UPDRS subscale IVa scores indicated that changes in severity and duration of dyskinesia did not reach significance in any group. The IGA of dyskinesia at month 3 showed that dyskinesia increased in 9% of patients receiving placebo, compared with 32% in the 100 mg tolcapone tid group and 40% in the 200 mg tid group. Decreased dyskinesia occurred in 7% of patients in the placebo group, 16% in the tolcapone 100 mg tid group, and 18% in the 200 mg tid group.
Additional analyses were performed to assess the temporal characteristics of the prevalence rate of the adverse events dyskinesia and diarrhoea. Analysis of the prevalence of dyskinesia at monthly intervals for the first nine months of the study (fig 3) shows that the risk of dyskinesia was highest in the first 29 days of the study in all three groups; thereafter the risk decreased dramatically in all groups between days 30 and 59. After day 59, only eight new cases of dyskinesia were reported: four in the 100 mg tolcapone tid group, two in the 200 mg tid group, and two in the placebo group. Similarly, analysis of the prevalence of diarrhoea during the first nine months of the study (fig 3) shows that the risk of developing diarrhoea decreased with time in both tolcapone groups. Of the nine cases of diarrhoea reported in the 100 mg tolcapone group, the onset of four cases was reported in each of months 1 and 2. Of the 15 cases reported with 200 mg tolcapone tid, five started in month 1, four in month 2, and four in month 3. Analysis of the hazard rates showed that, with 100 mg tolcapone tid, the risk of developing diarrhoea was about 7% during the first 59 days of treatment, hereafter the risk decreased; no new cases were reported after day 89. With 200 mg tolcapone tid, the risk was about 8% until day 89, hereafter it decreased; no new cases developed after day 179. No treatment related differences in vital signs and ECG results were found between the study groups. For most laboratory tests, mean values at baseline and all assessment points and mean changes from baseline were similar for all treatment groups. However, with 200 mg tolcapone tid, mean concentrations of aspartate aminotransferase (AST) and alanine transferase (ALT) were higher at week 6 than with placebo, before reverting to baseline values for the remainder of the study. Highly abnormal ALT concentrations were found in three patients (one in the 100 mg tolcapone tid group, two in the 200 mg tid group), all of whom had concomitantly high AST concentrations. One of these patients (from the 200 mg tolcapone tid group) withdrew on day 113 of the study because of raised liver transaminases. At an assessment on day 118, this patient’s ALT concentration was 103 μm/l and AST was 41 μm/l; both transaminase activities declined gradually thereafter until AST was within the standard reference range by day 147 and ALT by day 169. This patient was the only one to withdraw from the study because of pronounced laboratory abnormalities; these were considered by the treating physician to be probably related to tolcapone treatment.

{kind=link}
{kind=link}
{kind=link}
Prevalence rates of (A) dyskinesia and (B) diarrhoea up to month 9. Rates are presented as the percentage of patients reporting these adverse events at the specified intervals.
Discussion
The present study confirms and extends previous findings28 29 that tolcapone enhances the efficacy of levodopa. Whereas initial studies were focused on single dose6 or short term (one to six weeks) multiple dose22 26 coadministration of tolcapone with levodopa/decarboxylase inhibitor, the present study showed that multiple dose (tid) treatment with tolcapone results in reduced severity of “wearing off” type motor fluctuations in levodopa treated patients for three months and that this response is maintained over time.
Treatment with tolcapone significantly decreased mean “off” time (by >20%) and increased mean “on” time (by >25%), compared with placebo. Analysis of primary end point “on/off” data disclosed that both tolcapone dosages were equally effective in increasing “on” time, but the 100 mg tid dosage was more effective in decreasing “off” time. However, the mean reduction in levodopa dosage by month 3 was greater with 200 mg tolcapone tid than with 100 mg tid This reduction was maintained until the nine month end point only with the higher tolcapone dosage; possibly the failure to find significant results at this point was due to the smaller sample size.
A small but significant reduction (compared with placebo) in UPDRS motor and total scores and in quality of life measures (SIP total and psychosocial scores) was found at month 3 with 200 mg tolcapone tid. The IGA of effficacy also showed significant overall improvements in efficacy of treatment with both tolcapone dosages.
Although an increase in “on” time would, by implication, lead to increased duration of dyskinesia, the overall proportion of patients exhibiting levodopa induced dyskinesia of a particular duration or intensity did not increase with either tolcapone dosage. This is most likely a reflection of the concomitant decreased levodopa dosage in patients treated with tolcapone. In addition, although dyskinesia occurred early in the study, the incidence in the tolcapone treatment groups diminished substantially with time before plateauing just above the incidence in the placebo group. Moreover, the risk of developing new dyskinesia decreased dramatically after the first month of treatment. Further studies are required to elucidate more fully any association between tolcapone and levodopa induced dyskinesia because the present study was not designed to quantify dyskinesia optimally.
Previously at these dosages, tolcapone had been shown to increase levodopa bioavailability up to twofold,6 so an increase in levodopa induced adverse events was expected. However, only 12 patients treated with tolcapone altogether withdrew from the trial because of adverse events induced by levodopa, so these were not considered to be treatment limiting.
Diarrhoea, which was reversible in all cases, was the most often reported non-dopaminergic event and the most often cited reason for premature withdrawal: 10 patients altogether withdrew because of diarrhoea, which resolved soon after stopping treatment with tolcapone. The incidence of diarrhoea was related to tolcapone dosage. However, patients reporting diarrhoea in the tolcapone groups usually did so early in the study, and the prevalence rate of diarrhoea decreased with time, indicating that patients who had not developed diarrhoea during the first six months of treatment were unlikely to experience it thereafter. This side effect has been found to occur with another second generation COMT inhibitor, entacapone.30 The mechanisms responsible for diarrhoea induced by COMT inhibition are under investigation.
Raised liver transaminases were found in only three patients, and, although the abnormalities were considered to be probably related to tolcapone treatment, only one patient withdrew from the study for this reason. This patient was asymptomatic, and enzyme concentrations returned to normal within about one month after treatment was withdrawn. The underlying mechanism leading to this adverse event is also unclear; the transaminase abnormalities found in the other two affected patients resolved without sequelae while they were still receiving tolcapone.
In summary, tolcapone was significantly more effective than placebo in reducing the “wearing off” phenomenon and improving overall clinical status and treatment efficacy in parkinsonian patients treated with levodopa. Both dosages seemed equally effective according to the primary efficacy measure (changes in “on/off” time), although secondary efficacy results (UPDRS and SIP scores) suggested that 200 mg tolcapone tid was more efficacious. However, the larger dosage was associated with greater incidences of adverse effects and premature withdrawals. Additional studies are needed to ascertain which dosage will provide optimum long term benefit: risk ratios in fluctuating patients. Results obtained in this study suggest that a tolcapone dose of 200 mg tid is not as well tolerated as the smaller dose and should only be used if a satisfactory improvement is not attained with 100 mg tolcapone tid The present study nevertheless provides evidence that tolcapone addresses the need for an agent that compliments current antiparkinsonian therapy, by extending the period during which levodopa is effective.
This study was supported by F Hoffmann-La Roche Ltd, Basel, Switzerland.It has been published as a condensed version in the Proceedings of the 4th International Congress of Movement Disorders, Berlin: Springer-Verlag, 1996
Appendix
The study investigators were: E Auff, Vienna, Austria; D Volc, Vienna, Austria; E Dupont, Arhus, Denmark; B Mikkelsen, Hjoring, Denmark; L Wermuth, Odense, Denmark; J Womm-Petersen, Gentofte, Denmark; H Baas, Frankfurt, Germany; R Benecke, Dusseldorf, Germany; T Eichhom, Marburg, Germany; H Kolbe, Hannover, Germany; W Oertel, Marburg, Germany; W Poewe, Berlin, Germany, and Innsbruck, Austria; G Ransmayr, Innsbruck, Austria; K Schimrigk, Homburg, Germany; A G Beiske, Nordbyhagen, Norway; J-E Olsson, Linkoping, Sweden; S Palhagen, Jonkoping, Sweden; J-M Burgunder, Bern, Switzerland; A Ghika, Lausanne, Switzerland; F Regli, Lausanne, Switzerland; A Steck, Basel, Switzerland; M Jackson, Birmingham, UK; P Medcalf, Dorset, UK.