Article Text

Abstract
The gene for myeloperoxidase (MPO) has been implicated in multiple sclerosis (MS). By measuring H2O2 dependent oxidation of 3,3′5,5′-tetramethylbenzidine with spectrophotometry the authors investigated MPO activity in peripheral blood leucocytes from 42 patients with MS (12 with secondary progressive MS, 17 with primary progressive MS, and 13 with relapsing remitting benign MS) and 32 healthy controls. Leucocyte MPO activity was significantly lower in patients with benign MS (mean (SEM) 0.086 (0.029) U/mg protein; p<0.01), secondary progressive MS (0.038 (0.009) U/mg protein; p<0.001), and primary progressive MS (0.057 (0.016) U/mg protein; p<0.001) compared with healthy controls (0.322 (0.053) U/mg protein). These data suggest that low MPO, which may be genetically determined, plays a part in MS pathogenesis.
- multiple sclerosis
- myeloperoxidase
- MPO, myeloperoxidase
- MS, multiple sclerosis
- EAE, experimental allergic encephalitis
- BMS, benign multiple sclerosis
- SPMS, secondary progressive multiple sclerosis
- PPMS, primary progressive multiple sclerosis
Statistics from Altmetric.com
- MPO, myeloperoxidase
- MS, multiple sclerosis
- EAE, experimental allergic encephalitis
- BMS, benign multiple sclerosis
- SPMS, secondary progressive multiple sclerosis
- PPMS, primary progressive multiple sclerosis
Myeloperoxidase (MPO) is a lysosomal enzyme present in neutrophils, monocytes, macrophages, and microglia.1–3 In human neutrophils it is part of the host defence system against invading micro-organisms. MPO catalyses the formation of hypochlorite anion-radical (OCl−.), as well as other cytotoxic oxidants, which have a potent activity against a wide range of bacteria, viruses, and fungi.1 The role of MPO in microglia is uncertain, but might be similar. There is growing evidence that MPO may also influence non-infectious conditions, including atherosclerosis, lung cancer, and Alzheimer’s disease.1
The chromosome 17q22–23 region, which includes MPO at 17q23.1, was independently identified in two genome screens as having a weak linkage with MS.4,5 By using additional microsatellite markers selected on nearby candidate genes, a marker related to the MPO gene revealed tentative evidence for linkage disequilibrium.6 A few studies have investigated −463 G/A MPO promoter polymorphism in multiple sclerosis (MS). Nagra and coworkers found an overrepresentation of the GG genotype in women with early onset MS.2 Two subsequent studies found no association between MPO promoter polymorphism and MS.7,8 Experimental allergic encephalitis (EAE) is an inflammatory disease of the central nervous system, which serves as an animal model for MS. Compared with wild type littermates, MPO knockout mice had significantly increased incidence of EAE.9
Considering a potential role of MPO in MS we investigated leucocyte MPO activity in patients with different subtypes of MS and healthy controls.
PATIENTS AND METHODS
The study was approved by the medical ethics committee of the University Hospital Groningen. Venous blood was obtained from 32 healthy controls and 42 patients with clinically definite MS.10 There were 13 patients with relapsing remitting benign MS (BMS), 12 with secondary progressive MS (SPMS), and 17 with primary progressive MS (PPMS). BMS was defined as an Expanded Disability Status Scale (EDSS) score of 3.0 or less despite at least 10 years of disease duration. The term PPMS was used for patients in whom the disease was characterised by a progressive course from the onset, without superimposed exacerbations. Exclusion criteria were the presence of infections or fever, and a relapse or the use of corticosteroids within the past three months. Six patients were using interferon beta. No other immunomodulatory or immunosuppressive drugs were used by any of the patients. Demographic data of patients and controls are given in table 1.
Demographic data
Isolation of leucocytes
Peripheral venous citrated blood was obtained through an intravenous cannula in the forearm. Leucocytes were isolated according to the method of Percy and Brady.11 Red cells were allowed to sediment in 1 ml dextran 5% for 90 minutes at room temperature. The leucocyte rich upper layer was removed and centrifuged (150 g) for 10 minuts at 4°C. The supernatant was removed and reaming red cells were lysated in NH4Cl (0,155 M), KHCO3 (0.01 M) and disodium EDTA (0.001 M). The pellet was centrifuged (150 g) twice for five minutes at 4°C. The leucocytes were washed four times in 2 ml NaCl 0.9% and centrifuged (150 g) for five minutes at 4°C. The final suspension of leucocytes was mixed with 2 ml of aqua bidest, and the lysated leucocytes were kept at −20°C until used.
Measurement of leucocyte MPO activity
Leucocyte MPO activity was assessed by measuring the H2O2 dependent oxidation of 3,3′5,5′-tetramethylbenzidine (TMB).12 The reaction was measured in a Beckmann DU-65 spectrophotometer. The reactive mixture contained 2.1 ml of buffer based (0.1 M potassium phosphate buffer, pH 5.4) solution of H2O2 (0.1 mM), 0.6 ml of the same buffer and 0.1 ml of TMB (1.6 mM). The reaction was started by adding 200 μl of suspension of leucocytes (at a protein concentration of 0.15–0.20 mg/ml), and absorbance was measured every minute for four minutes. One unit of enzyme activity was defined as the amount of MPO present that caused a change in absorbance of 1.0/min at 655 nm and 25°C.
Statistics
The significance of between group differences was assessed using the Kruskal-Wallis test. Only when these results were significant were comparisons between specific groups done using Dunn’s multiple comparisons test. The Mann-Whitney test was used for comparison of two groups. Statistical significance was taken to be at the 5% level (p<0.05).
RESULTS
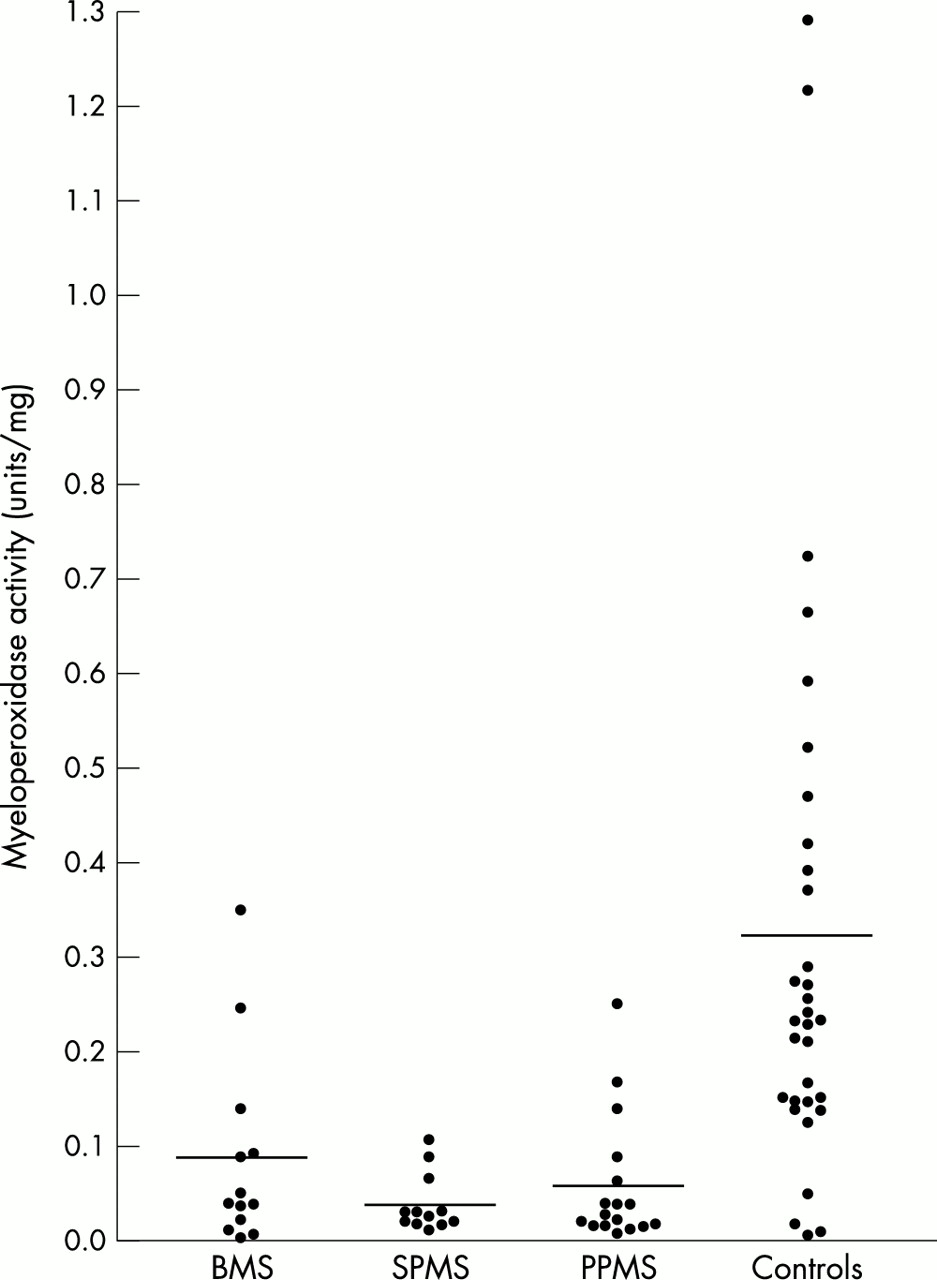
There were significant differences in mean leucocyte MPO activity between the four groups (healthy controls, BMS, SPMS, or PPMS; p<0.0001; fig 1). Mean (SEM) leucocyte MPO activity in controls was 0.322 (0.053) U/mg protein. Compared with controls, mean leucocyte MPO activity was significantly lower in patients with BMS (p<0.01), SPMS (p<0.001), and PPMS (p<0.001) (table 1). There were no significant differences in mean leucocyte MPO activity between BMS, SPMS, or PPMS. No significant association was found between the use of interferon beta and leucocyte MPO activity (0.071 (0.039) compared with 0.061 (0.012) U/mg protein; p=0.774).
{kind=link}
Leucocyte MPO activity in healthy controls, patients with relapsing remitting benign MS (BMS), secondary progressive MS (SPMS), and primary progressive MS (PPMS). The transverse solid lines represent the mean value. There were significant differences (p<0.0001; Dunn’s multiple comparisons test) between controls and each of the three subcategories of MS.
DISCUSSION
This study shows low MPO activity in peripheral blood leucocytes in patients with MS compared with healthy controls. This is in contrast with other diseases, such as arteriosclerosis, lung cancer, and Alzheimer’s disease, where high MPO activity is linked to abnormality through its strong oxidative activity.1 Our data consistently show low MPO activity in three subgroups of MS characterised by a different clinical course (BMS, SPMS, and PPMS). The significance of our finding is at present uncertain. Low MPO activity might be secondary to the disease process occurring in MS, or play a part in the pathogenesis of MS.
Epidemiological data support a role of one or more infectious agents in the aetiology of MS. Because MPO is part of the host defence system against invading micro-organisms, high enzyme activity could protect against infectious agents that may be implicated in MS. High MPO activity could also protect against MS because it down regulates immunopathological mechanisms. This possibility is supported by studies in EAE, which is an animal model of inflammatory demyelinating disease of the CNS. Brennan and coworkers studied the incidence of EAE in mice immunised with MOG35–55 peptide.9 They detected MPO in invading macrophages in the CNS of wild type mice. However, unexpectedly, MPO knockout mice had significantly increased incidence of EAE. Only 7% of the MPO knockout mice were resistant tot EAE symptoms, as compared with 57% of wild type littermates. Throughout the observation period MPO knockout mice exhibited more severe disease; 90% of MPO knockout mice developed complete hind limb paralysis as compared with 33% of wild type littermates. These findings indicate that low MPO activity may facilitate the development of EAE, and our data suggest that a similar phenomenon might occur in MS.
T cells reactive to myelin antigens, including myelin basic protein, proteolipid protein, and oligodendrocyte glycoprotein are present in the peripheral blood of both MS patients and healthy people.13–15 Once activated these T cells have the ability to traffic into the CNS and search for target antigens. Anti-myelin T cells can be activated in the periphery by cross reactions with a wide range of common viral antigens,16 and people with MS have similar exposures to common infections as healthy people do. Clonal expansion of anti-myelin T cells, indicating their activation, has been observed both in patients with MS and healthy people.17 These data suggest that regulatory mechanisms that down regulate potentially pathological T cell responses may be defective in MS. Evidence indicates that MPO plays a part in down regulating autoimmune responses. In the EAE model, Brennan and coworkers found that the proliferation rate of T lymphocytes in MPO knockout mice was 1.5-fold higher than in wild type littermates.9 The oxidant hypochlorus acid produced by MPO activity reacts with taurine, a free amino acid abundantly present in most mammalian tissues,18 to form taurine chloramine, which is a long lived molecule with immunomodulatory properties. Taurine chloramine suppresses the proliferation of human lymphocytes, inhibits the generation of proinflammatory cytokines such as tumour necrosis factor α, interferon gamma, and interleukins 6 and 12, and increases the production of the anti-inflammatory interleukin 10.19–21
If low MPO activity plays a part in the pathophysiology of MS it may be genetically determined. Interestingly, the syntenic region of murine chromosome 11 (57–52 cM), including MPO at 49 cM, is also a susceptibility locus for EAE.22 Two genome screens suggested a link between the chromosome 17q22–23 region, which includes MPO at 17q23.1, and MS.4,5 Cellular levels of MPO can be influenced by a functional promotor polymorphism, which precedes the MPO gene. No convincing association has been found between MS and −463 G/A MPO promoter polymorphism.7,8 However, recently another MPO promoter polymorphism, −129 G/A, has been discovered.23 Further research in MPO promotor polymorphisms and leucocyte MPO activity in MS is warranted.
Acknowledgments
We are indebted to Natasha Maurits for her help in the statistical analyses and to Michael G Stepanov, Reint Hartman, and Koos Roggeveld for their help in the laboratory measurements.
REFERENCES
Footnotes
-
Funding: this work was supported by Multiple Sclerosis Internationaal (MSI), Amsterdam.
-
Competing interests: none declared.