Article Text

Abstract
Result of the immunohistochemical reactions routinely used in diagnostic surgical pathology should be properly interpreted, since false results, related to technical and interpretative pitfalls may lead to incorrect diagnosis. The main sources of such pitfalls are reviewed, analytically described and related to different steps (fixation, tissue processing and embedding, decalcification, antigen retrieval) which may affect the accuracy of immunohistochemistry. In addition, the presence of endogenous enzyme activity, improper binding of avidin to endogenous biotin, incorrect use of antibodies, chromogen and detection systems, as well as incorrect interpretation may produce unreliable data. The high frequency and extension of such pitfalls make mandatory the use of internal and external controls and adoption of cross-validation programmes. The present study, supported by an extensive review of the related literature, is intended as a guideline leading to proper interpretation of immunohistochemical data, an essential component of the diagnostic process. Experience on the antigen retrieval procedures for different antigens is also presented.
Statistics from Altmetric.com
Immunohistochemical staining has become an essential complement to morphological analysis in histocytopathology diagnosis. Pathologists should therefore become familiar with technical and interpretive pitfalls, since many factors may influence the technical preparation of the immunoreactions and a wide variety of causes can result in incorrect interpretations (see table 1). Variables affecting immunostaining may involve different steps of the routine technical tissue processing, such as the fixation procedure (type, duration, temperature, and pH of the fixative), the dehydration and embedding processes, or factors causing loss of antigen, such as tissue necrosis and changes in the level of antigen expression. Other factors are more specifically related to immunohistochemical methods, such as specificity and sensitivity of the antibody, buffer solutions, detection system, chromogen and antigen retrieval systems. Finally, we should consider the possible pitfalls connected to insufficient familiarity with the immunohistochemical microscopic pattern of the different diagnostic and prognostic markers.
The present study is a review of the technical pitfalls, which may hamper interpretation by histopathologists of immunohistochemical staining results in paraffin-embedded tissues specimens.
FIXATIVES
Length and type of fixation may influencer immunohistochemical staining. In order to block autolysis (hence loss of protein reactivity), surgical biological samples should be reduced in small blocks as soon as possible and then placed in fixative. Drying of specimens (especially at the surface of tissue blocks) may result in non-specific staining, since any antibody may non-specifically attach to dried tissue as a result of local ionic charges.
Two types of fixatives are used in histopathology—cross-linking fixatives, such as formalin, and coagulating fixatives, i.e. alcoholic solutions; both may cause pitfalls.
The length of fixation can affect the results of the immunostaining1–3 as under-fixation often produces a reduced immunostaining in the central region of the tissue block with stronger immunoreaction in the marginal area of the section, while overfixation generates the opposite effect (good staining in the inner area and poor staining outside).1–3 Specifically, under-fixation in formalin can affect oestrogen receptor determination in breast cancer and a minimum fixation time of 6 hours is regarded as mandatory for obtaining reliable results.142
Protracted formaldehyde or glutaraldehyde fixation may also generate free aldehyde groups in tissues with the effect of a non-specific binding of conjugated antibodies (false positive staining).3 This problem can be abolished using different blocking solutions, such as sodium borohydride, ammonium chloride, ammonium carbonate buffer, lysine and glycin.4 Moreover, formaldehyde fixation modifies the conformation of macromolecules, altering tertiary and quaternary organisation of proteins, whereas the primary and secondary structures are not significantly affected.1 5 6 Such conformational changes may hamper the link to the antibody,7–9 but use of the antigen retrieval procedure can return immunoreactivity in formaldehyde-fixed specimens.9 The modifications produced by glutaraldehyde fixation are instead more stable and often permanent.10
Finally, if formalin does not penetrate the tissue completely during the fixation process, the subsequent use of ethanol (as a dehydrating agent) during paraffin embedding may produce in the tissue blocks central areas which are predominantly alcohol-fixed, and this can produce additional variable results.11 12
The typical coagulating fixative is ethanol, which removes water molecules and therefore destabilises hydrophobic bonding of the proteins, deploying their tertiary structure6 9 with the final outcome of protein denaturation. This process does not affect all the antigens, but most CD and some antigens particularly rich in carbohydrates may be deprived of their antigenicity. Moreover, inadequate cellular preservation of some growth factor peptides and a possible shift in intracellular immunoreactivity has been reported.13–15
A wide variability in reactivity has been observed using alternative fixatives.9 10 12 Mercury-based fixatives, such as B5 and Zenckers are fixatives used particularly for haemolymphoproliferative pathology since they provide excellent nuclear morphology.12 Similar to formalin, mercury-based fixatives induce molecular cross-linking, but to a larger extent than aldehyde solutions, and as a result may hamper reactivity of a number of important antigens, for example CD4, CD5, CD10, CD23 and sometimes CD30.14–16 On the contrary, κ and λ light chains perform better in B5 than in formalin-fixed tissues.14 In addition, using these fixatives it is necessary to remove precipitated pigment; it has been argued that denaturation of the antigens can be caused by reagents employed for such a purpose, i.e. by Lugol’s iodine or similar solutions.17
TISSUE PROCESSING AND EMBEDDING
The steps of processing and embedding of tissues seem to have less influence than fixation on the results of immunohistochemical procedures. However, dehydration has been shown to influence the preservation of some antigens and special attention should be given to the embedding procedures.18 Care should be taken in controlling the temperature of paraffin wax, since an increase of the temperature above 63°C and extended periods of dehydration, paraffin embedding and heating above 68°C during attachment of sections to microscope slides may cause loss of reactivity of some antigens such as PCNA.18–20 Moreover, it has been suggested that the combined effect of formalin with heat and non-polar solvents used in paraffin infiltration may change the conformation of some antigens.18 In some cases, it has been hypothesised that fixation alone does not prevent immunolabelling, whereas tissue processing is the restrictive factor.18–20
It is common experience that in very old tissue blocks some antigens, such as Ki67, ER and HER2 show loss of reactivity. The reason for this is unclear: interference of paraffin is unlikely since, as the name implies, paraffin has no affinity for other chemicals. In our opinion, a slow protraction of the cross-linking reactions of formaldehyde, with a progressive transformation of aminomethylol groups to the more stable methylene bridges seems more likely. In such cases, results can still be obtained by an enhancement of the retrieval procedures.
DECALCIFICATION
Decalcification may affect antigen preservation, which may be reduced. In some studies no significant changes have been reported when decalcification was performed using EDTA.21–23 A good quality of morphology and immunohistochemistry has been reported using a mercuric chloride–formaldehyde fixative solution and 10% acetic acid decalcification,24 while decreased antigenicity may be observed when 10% formic acid or 5% nitric acid is applied.21–23 Some authors reported no significant loss of immunostaining even when strong acids were used.25 In our experience decalcification by strong acid on bone and bone marrow samples has a negative effect on the detection of most antigens, particularly CD markers. This is in agreement with most of the reported studies.26–28
ANTIGEN RETRIEVAL
Modifications of the tertiary structures of the antigens may prevent binding to the specific antibody29 and for this reason different retrieval procedures were developed, and tailored on formalin-fixed tissues.30–36 It is well known that the requirement of the retrieval procedures is related not only to the antigen and the specific epitope to be detected but also to the type of the antibody.30 In fact, polyclonal sera perform better than monoclonal antibodies, which bind to a single epitope.30
Huang37 38 initially set up the enzyme or protease induced epitope retrieval (PIER), and many studies have been reported describing different procedures using various enzymes.39–43 Even if the exact mechanism of PIER is still unknown, non-specific cleavage of the protein was hypothesised.44 PIER may produce many pitfalls, because some epitopes might be lost,44 and it is noteworthy that the action of such treatment is related to the type, to the titre and to the incubation procedures (i.e. time, temperature and pH) of the enzyme.39 41 43 Moreover, PIER is influenced by the length of fixation.44 As a downside of this procedure, destruction of the antigens may be observed.42 44
The original observation by Fraenklen-Conrat et al45–47 that the methylene cross-links between proteins and aldehydes can be partially disconnected by high temperature or strong alkaline hydrolysis, prompted Shi et al29 to introduce the concept of “antigen retrieval”. Heating by a microwave procedure can reveal masked antigens, but the precise mechanism of action of the heat-induced epitope retrieval (HIER) is still largely unknown, although many investigations have been carried out.48–54
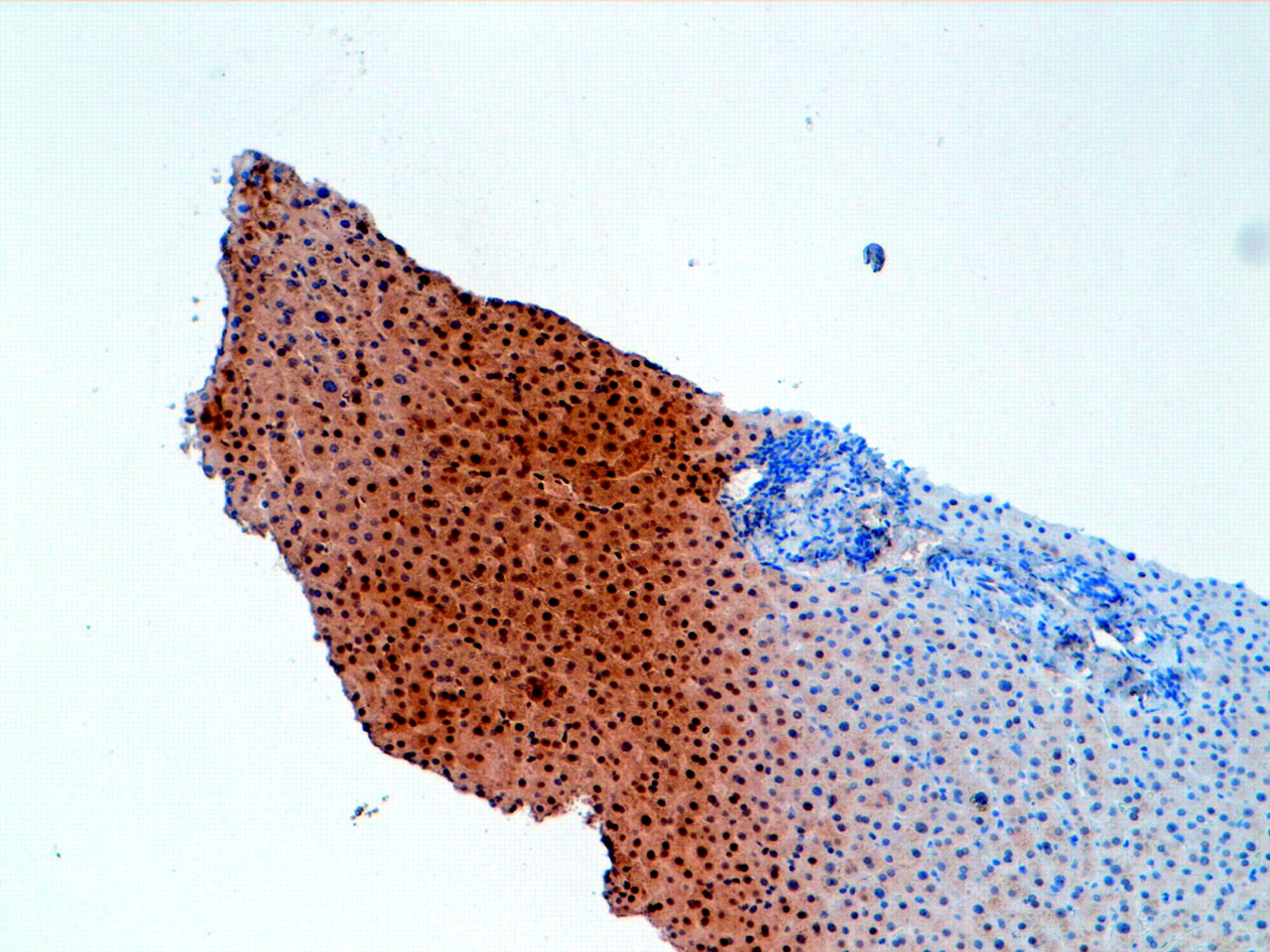
Some cross-links are completely reversible (i.e. Schiff bases), whereas not all the methylene bridges are broken.44 In addition, the length and type of fixation can modify the antigen reactivity following HIER, since it has been observed that formalin seems to protect the antigens from the temperature denaturation, while most of the unfixed proteins are denatured at 70–90°C.3 55 The type of retrieval buffer and the pH of the solution are also important in order to prevent false results.35 56 57 Some antigens benefit from a low pH solution, while others can be retrieved only when a high pH solution is employed.1 55 58 Several antigens, including CD20, cytokeratins, EMA, NSE and PCNA display no significant variation at pH values ranging from 1.0 to 10.0, while other antigens (for example, MIB1 and ER) exhibit instead a remarkable decrease in staining intensity using pH values ranging from pH 3.0 to 6.059–61 (fig 1).

The molarity of the solution may also significantly influence immunostaining.62 EDTA solutions are more effective than citrate buffer for some antigens,63–66 but the unmasking effect of calcium buffered solutions cannot be recognised for other markers.67 68
The time of action and the power of the microwave (or the temperature) play an important role in the process of HIER,69 70 and usually such variables are inversely related. It has been observed that to obtain the same retrieval effect, antigens need a higher temperature for a short time or a lower temperature for a longer time.29
HIER, when used for inadequate time and temperature (or microwave power) can generate different pitfalls: unmasking of the antigen, creation of new antigenic binding sites, or the exposure of endogenous biotin in formalin-fixed tissues.71 Moreover, not all the antigens can be effectively retrieved by means of HIER, especially after prolonged formalin fixation.50 72
Antigen retrieval procedures vary in different laboratories according to local experience, so that different protocols, specific for the various antigens, have been selected. Our personal experience was developed in separate laboratories (dealing with a total of approximately 30 000 immunohistochemical tests/years). Such experience (which occasionally varies for single antigens) can be viewed online (www.oncologiaumana.unito.it/treatments/). Readers may refer to our suggestions for antigen retrieval methods.
ENDOGENOUS ENZYME ACTIVITY
Endogenous peroxidase activity, which is physiologically present in many cells, such as erythrocytes, granulocytes and neurons, can react with the chromogen, thus producing a staining identical to specific immunoperoxidase19 73–76 (fig 2). Fixation and embedding processes reduce endogenous enzymatic activity, but the residual tissue activity must be completely blocked so as to prevent false positivity.19 73–76 Tissues with high blood content (e.g. site of heavy haemorrhage), thus rich in haematin or with intense granulocytic inflammatory infiltrate, need a stronger solution in order to suppress endogenous peroxidase, but this procedure is not to be recommended for specimens in which cell surface antigens, such as CD4, are to be detected.19

Endogenous alkaline phosphatase is also destroyed during routine formalin fixation and processing,19 and it should be noted that the use of alkaline phosphatase in immunohistochemistry avoids most of the problems related to endogenous peroxidase activity.77
Effects of avidin and biotin
Egg white avidin binds to nucleic acids, phospholipids, and glycosaminoglycans by its high ionic attraction,7 78 but this non-immune attachment can be prevented using solutions at pH 9.4.79 80 Such non-specific binding is significantly reduced when using streptoavidin (from Streptomyces avidinii) instead of avidin.79 81–84
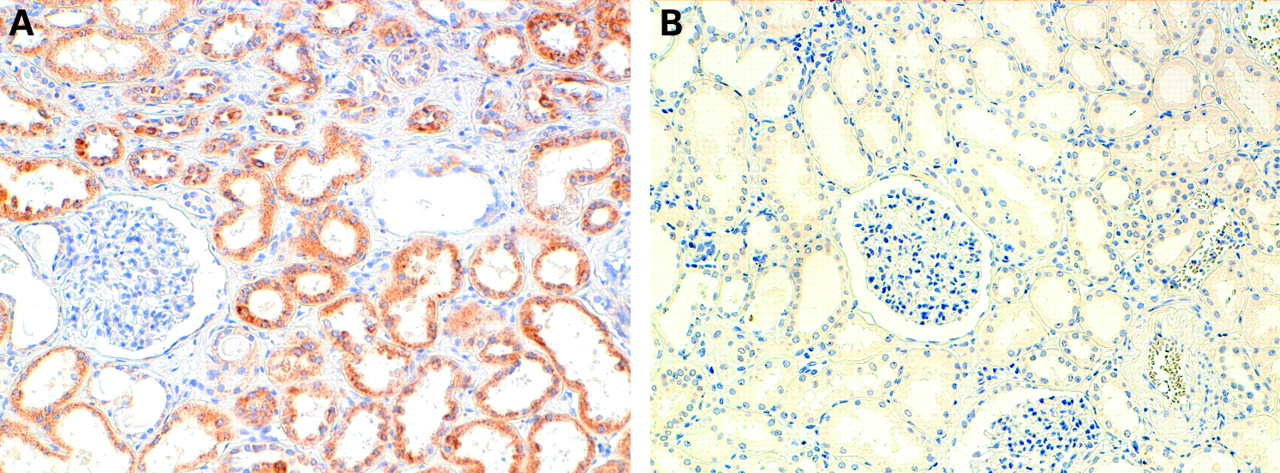
A strong background and false positive results can be produced by the binding of avidin used in detection systems to endogenous biotin. It is well known that endogenous biotin is widely distributed in human tissues, particularly in liver, lung, spleen, adipose tissue, mammary gland, kidney (fig 3) and brain.71 80–84 Formalin fixation partly blocks the reactivity of endogenous biotin (a coenzyme), but HIER procedures retrieve its reactivity, thus causing a potential pitfall, which can be prevented by selective blocking.19 80 85–87 Gestational and postpartum endometrial cells can represent a potential pitfall, since they can have endogenous intranuclear biotin inclusions that may be mistaken for positive viral inclusion when immunohistochemistry is carried out for viral antigens.88–91 Similar pitfalls can occur in some neoplastic cells, above all after HIER treatment92–94; failure to recognise this artefact may be responsible for incorrect immunohistochemical diagnoses.95 96

Other examples of endogenous avidin-binding activity include the non-specific staining of myelin97 and mast cells in both frozen and paraffin-embedded tissue.79 98
PRIMARY ANTIBODIES
Ionic interactions and hydrophobic forces play a significant role in antigen–antibody binding, but they can also generate unacceptable background.99 Although fixation is considered the most important factor influencing preservation of the antigen, the buffer in which the antigen–antibody reaction takes place might have some effect on the binding.19 29 100 Immunoglobulins can have either positive or negative charges at the pH of the buffer usually employed as diluents101; ionic interactions between the antibody and tissue proteins may therefore occur.100 Non-specific reactions to nuclear proteins can be observed after antigen retrieval by zinc sulphate, citrate (pH 6.0) and Tris (pH 9.0) buffer solutions. The reason for this non-specific nuclear staining is still unknown, but it has been assumed that a combination of electrostatic and polar interactions forces are involved.100–103 In our experience, extensive rinses before immunocytochemical procedures can prevent such spurious staining.
Another cause of non-specific tissue staining can be related to an inadequate storage of the reagents: hydrophobicity increases as a result of polymerisation and aggregation of the immunoglobulins and produces an increase of background staining.104 This phenomenon is amplified when the antibodies are biotinylated.105
Interaction between the antibody conjugate and the protein polar groups in tissue sections also generates background.104 Another source of background is the complement-mediated binding of antibodies to tissue proteins when whole polyclonal antisera are used.106 In addition, non-specific, complement-mediated binding of sera to endocrine cells of the gastro-entero-pancreatic area has been reported; such spurious binding can be prevented by use of de-complemented sera.107
Non-specific staining can also occur because of attraction of the Fc fragment of the antibody to basic groups present in collagen fibres,108 or because of the binding of immunoglobulins to the cellular Fc receptors.19 109
A subtle relationship can thus be established between antibody titre, time and temperature of incubation in immunohistochemistry; hence, artefacts related to inappropriate antibody titres may occur. Antibodies used at a very low concentration (i.e. over-diluted) reduce the sensitivity of the assay and often lead to false negative results. On the other hand, conspicuous background is present when antibodies are used at high concentrations. However, the phenomenon of prozone must be considered: some antisera, when too concentrated, fail to bind to cellular antigens, while at a higher dilution they will do so. This event is primarily noted in antibody-induced agglutinations, but it can also be observed, although rarely, in immunohistochemistry.110
Adequate storage of the antibodies it is also essential. When bacteria begin to grow in the antibody solution or in other solutions, they give rise to finely granular clumps of chromogen deposition randomly scattered on the surface of the section.100
DETECTION SYSTEM
One critical point to be kept in mind using any detection system is to make certain that the detection complex is diluted in an appropriate stabilising buffer solution, because each enzymatic techniques needs specific pH solutions.19 111
Biotin-free techniques, such as the polymeric labelling two-step method, offer the advantage of a lack of background staining related to endogenous biotin or avidin.112–116 However, using this method it is possible to observe artefacts due to the ionic charges of the polymers, or false negative results related to spontaneous agglutination of the antisera.69 104
CHROMOGEN
If the chromogen is incompletely solved or not filtered before use, small traces of precipitate may be observed on the surface of the section. Moreover, simple variation in chromogen incubation times can produce vast differences in stain intensity that can severely affect microscopic evaluation.69
PITFALLS IN RESULT INTERPRETATION
Proper distribution of the signal revealing the subcellular distribution of the antigen inside the cell of interest (nuclear, cytoplasmic or membranous) is of major concern in interpretation.143 An aberrant location may be of pathological and diagnostic interest, but should be distinguished from a spurious staining.
When examining immunohistochemical stains of histological slides and cytologic smears, one must be aware that in some cases a certain amount of reagent “trapping” may occur. Non-specific antigen diffusion (fig 4) from the proper constituent cells and non-specific sequestration by other cells of different lineage or by the interstitium is a common problem, particularly observed with thyroglobulin, myoglobin, glial fibrillary acidic protein and other cellular proteins.117–119 144 Another pitfall is the spurious staining of cells phagocytosing other cells.120 When a high concentration of blood immunoglobulins permeates the tissue, before fixing, interstitial staining is frequently observed.100 121

Occasionally, small circular areas that lack immunoreactivity, an artefact formed by the production of bubbles in the reaction medium, may be detected.120 Likewise, air bubbles trapped under the section while drying can cause circular areas of heavy background staining.
Another cause of misinterpretation is originated by drying artefacts, produced if the reagents dry out during one of the incubations. Tissue sections may then appear with a diffuse monotonous colour, or there may be a total lack of immunostaining.69 100
Areas of trapped reagent can be produced by irregular folds in the histological sections or by small fragments detached from the slide as a consequence of HIER. Usually this artefact is found when the tissue is poorly fixed or remarkably sclerotic.69 122 123 In addition, cracks and spaces in tissue sections can show non-specific entrapment of reagents; in such spaces one can recognise a focal pattern of chromogen precipitation.69
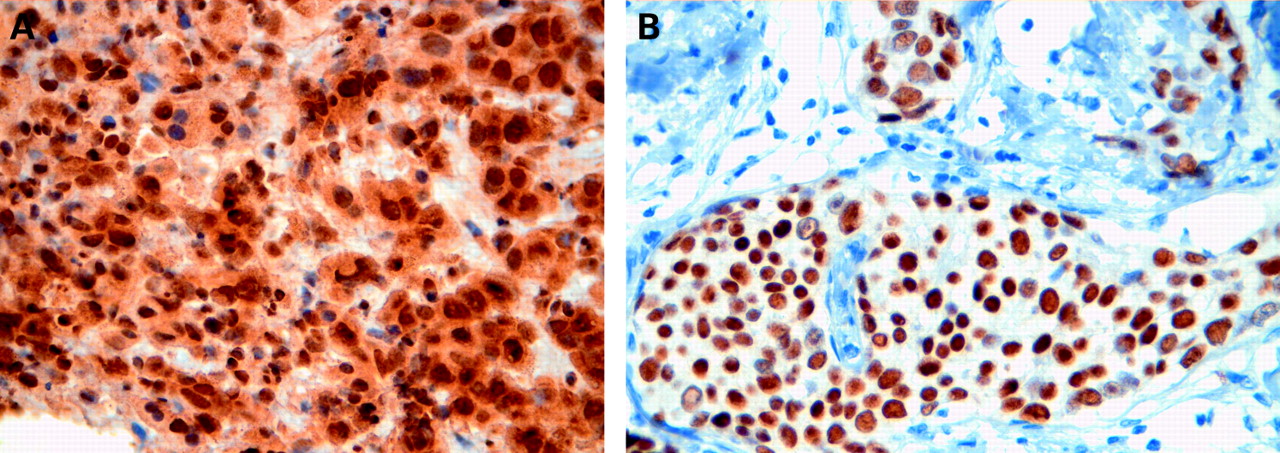
Cells that have been crushed during surgical procedures or tissue sampling may frequently show a non-specific immunostaining regardless of the antibody used.124 Similar pitfalls may be observed in necrotic or haemorrhagic areas,69 75 while necrotic and apoptotic cells often show false positive staining due to oxidative enzymes.69 The same phenomenon occurs in lysosome-rich cells, for example in granular cell tumours, because of the presence of a large amount of oxidative enzymes within the lysosomal bodies.69 Mitochondria-rich cells, such as in oncocytomas (fig 5), may also show non-specific immunostains.69 RNA-rich cells in the stratum granulosum of the epidermis may also show false positive immunoreactions.69

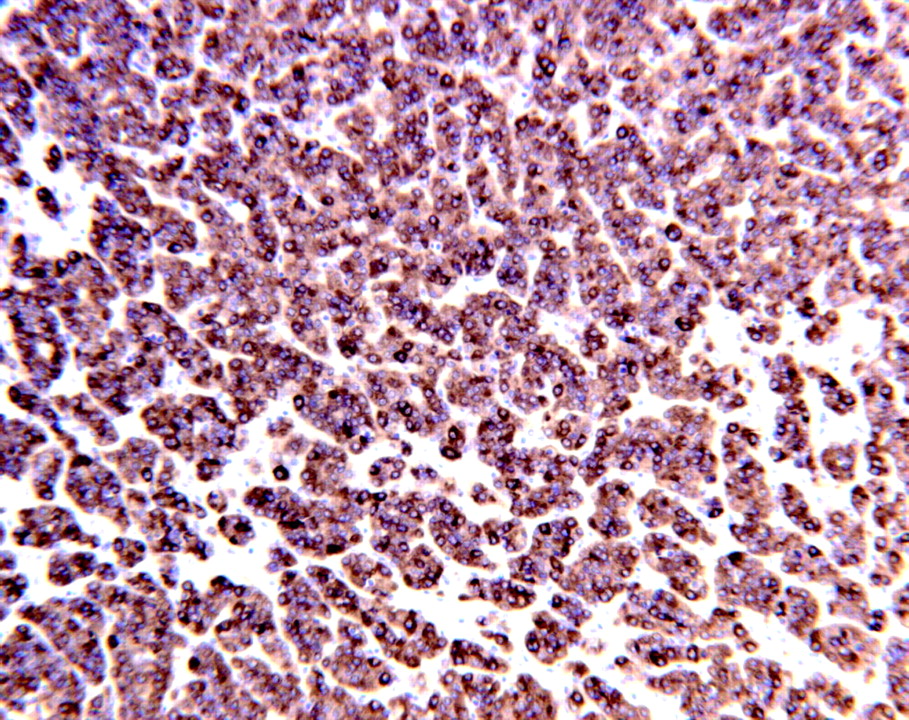
The free edge of histological sections and the surface membrane of isolated cells may sometimes display a false positive reaction124 (fig 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pathologists should, on the other hand, be aware that immunohistochemical results interpreted in many cases as “aberrant” antigen appearance are in fact related to proper antigenic expression, as proved by molecular investigations. For example, cytokeratin positivity can be detected in mesenchymal tumours, such as angiosarcoma, leiomyosarcoma and rhabdomyosarcoma,69 125–127 and the cytoplasmic and/or cell membrane localisation of ALK in an anaplastic large cell lymphoma should not be interpreted as a false-positive reaction, since it is a characteristic of a variant form of the ALK fusion protein, different from the usual nuclear location.128–130
Sometimes the “aberrant” localisation of the immunoreaction can even be used as a diagnostic tool. For example, in hyalinising trabecular thyroid tumour (HTT) a membrane pattern distribution of Ki67 antigen (detected by clone MIB-1) immunostaining has been reported as typical of this tumour type and diagnostic, whereas the usual nuclear immunoreaction is seen when different antibody clones are employed.131–135 The presence of a partial antigen homology, possibly related to a peculiar neoplastic phenotype, seems a likely explanation. This is further supported by the fact that MIB-1 staining of tumour cell membranes is restricted to a subset of neoplastic lesions, including HTT cases and, occasionally, sarcomatous mesothelioma, invasive breast carcinoma, and renal oncocytoma.131
Finally, pitfalls may be observed when studying cancer antigens, such as CA19.9, CA125 and CA150, since these markers display extensive cross-reactions and related antibodies are known to react to several normal and neoplastic epithelial cells of different origins.136–140
CONCLUSION
Immunohistochemistry has become an integral part of histopathological diagnosis and can provide essential data predictive of clinical evolution and of therapeutic responsiveness. Indeed, false-positive and false-negative results will impact on the management of patients affected by tumours, notably breast and colon cancer, haematological malignancies and gastrointestinal stromal tumours. Automatic processing has now become routine for immunohistochemical staining procedures, and this may give the false impression that the results are always totally reliable. There are however, many pitfalls which may affect the intensity and distribution of the staining.
Intricacies involved in the immunohistochemical determination of predictive markers in breast cancer are highlighted in a recent article in this journal.141 The present review specifically analyses the technical steps of the staining process and focuses on those pre- and post-embedding procedures (such as type and length of fixation and decalcification treatments) and on the antigen retrieval procedure which may alter the staining results, thus potentially affecting the pathological diagnosis.
Take-home messages
Pitfalls in immunohistochemistry may lead to incorrect interpretations and affect the diagnostic process.
The main factors potentially affecting immunohistochemical staining are tissue processing and antigen retrieval procedures.
Important (and often neglected) issues in immunohistochemistry are type and length of tissue fixation.
Insidious pitfalls are represented by the presence of endogenous biotin and enzyme activity.
Acknowledgments
The authors wish to thank Professor Giorgio Inghirami of Turin University for his helpful comments on the manuscript.
REFERENCES
Footnotes
Funding: This paper was supported by grants from Piedmont Region (Ricerca Sanitaria Finalizzata 2006).
Competing interests: None.