Article Text

Abstract
Background: There is a clear need to define biological markers that will predict the response to treatment in breast cancer, and several recent studies suggest that the expression of type 1 growth factor receptors may prove important in this regard. The type 1 growth factor receptors are a family of transmembrane receptors comprising epidermal growth factor receptor (EGFR), c-erbB-2, c-erbB-3, and c-erbB-4. Both EGFR and c-erbB-2 are associated with poor prognosis in certain tumours.
Aims: There is very little information concerning expression patterns of the full range of type 1 growth factor receptors, especially with respect to c-erbB-3 and c-erbB-4. Therefore, this study was designed to compare the expression of each, and to assess whether expression of any of the factors was related to patient survival in a clinical series.
Methods: Type 1 growth factor receptor expression was investigated by means of immunohistochemistry in a series of node positive patients with breast cancer (n = 66), and statistical analysis was carried out to determine associations between variables and survival analysis for each variable.
Results: There were several correlations between variables, and overexpression of EGFR, c-erbB-2, and c-erbB-4 was found to be associated with adverse clinical outcome, although the results were significant only for c-erbB-4 (p = 0.002).
Conclusion: Although patient numbers are small, this is the first report describing c-erbB-4 as an adverse prognostic marker. These findings are in contrast to previous investigations and may relate to the fact that the patients studied all had advanced stage disease and had undergone similar chemotherapy regimens in the context of a clinical trial.
- breast cancer
- type 1 growth factor receptors
- c-erbB-4
- prognosis
- immunohistochemistry
- CMF, cyclophosphamide, methotrexate, 5-flourouracil
- EGFR, epidermal growth factor receptor
- ER, oestrogen receptor
- NPI, Nottingham prognostic index
- NRS, normal rabbit serum
- PGR, progesterone receptor
- TBS, Tris buffered saline
- T1GFR, type 1 growth factor receptor
Statistics from Altmetric.com
- CMF, cyclophosphamide, methotrexate, 5-flourouracil
- EGFR, epidermal growth factor receptor
- ER, oestrogen receptor
- NPI, Nottingham prognostic index
- NRS, normal rabbit serum
- PGR, progesterone receptor
- TBS, Tris buffered saline
- T1GFR, type 1 growth factor receptor
The identification of prognostic and predictive factors in cancer is highly important in the identification and characterisation of tumours so that the optimum treatment can be given. In breast cancer, the main established prognostic factors are tumour size, grade, and stage, and all three factors are combined in many centres to give a predictive score using the Nottingham prognostic index (NPI).1
Although these general prognostic factors and the NPI are well established and can identify patients who may need more aggressive treatment, they can only provide a limited amount of information regarding the effects of specific types of treatment. Recently, however, there has been much interest in studying the expression of specific molecular markers in tumour cells, with the aim of identifying those that can determine response to specific types of treatment. In this regard, much current interest centres around the type 1 growth factor receptor (T1GFR) family.
This family comprises four known transmembrane receptors: epidermal growth factor receptor (EGFR), c-erbB-2, c-erbB-3, and c-erbB-4 (also known as HER1–4). Ligand binding to the external domain of these receptors triggers homodimerisation/heterodimerisation of receptors, which in turn stimulates tyrosine kinase activity from the internal domain. Numerous ligands have been defined that bind to EGFR, c-erbB-3, and c-erbB-4, but to date a specific ligand for c-erbB-2 has not been described.2
“Relatively little information exists regarding expression and prognostic relevance of the c-erbB-3 and c-erbB-4 receptors in different tissues and tumours”
Previously, interest in this family of receptors has centred primarily around c-erbB-2, which has become an established prognostic marker in breast cancer.2,3 Overexpression of this molecule is seen in 20–30% of breast cancers, and such patients have a generally poor prognosis, which in many cases may be a reflection of lack of response to conventional CMF (cyclophosphomide, methotrexate, 5-fluorouracil) treatment.4 Recently, c-erbB-2 has been targeted in trials of antitumour monoclonal antibody treatment using Herceptin®.5,6 This is a mouse–human chimaeric antibody that produces antitumour effects by blocking the c-erbB-2 receptor, and can also interact with tumour cells to effect antibody dependent cell mediated cytotoxicity. The T1GFRs possess tyrosine kinase activity, and this class of enzyme has recently shown promise as a target for antitumour treatment.7,8
Regarding the remaining members of the T1GFR family, EGFR expression has been shown to be associated with poor prognosis in some studies involving breast cancer,9,10 but overall it seems that the changes seen between normal breast and transformed breast epithelial cells are not significant.2 Relatively little information exists regarding expression and prognostic relevance of the c-erbB-3 and c-erbB-4 receptors in different tissues and tumours. Published studies of c-erbB-3 and c-erbB-4 expression and their association with clinical outcome in breast cancer show no consistent association with survival.11–15 Although Lemoine et al showed an association between c-erbB3 and positive lymph node status,12 two studies have failed to show an association with survival.11,13 A more recent study has shown an association between c-erbB-3 expression and factors associated with aggressive tumour behaviour.16 In the case of c-erbB4, several studies have shown an association with positive oestrogen receptor (ER) status17–19 or low grade,14 and studies on survival have shown either an association with better outcome19 or no association.14
In view of the overall lack of data concerning c-erbB-3 and c-erbB-4, and in particular studies that look at the importance of the receptor expression profile—for example, coexpression of c-erbB-2 with one or more other receptors—we have carried out an immunohistochemical study of expression of all four members of the T1GFR family in a series of 66 patients with breast cancer. We have analysed the data generated in our study with respect to relations between other biological variables, relations with established prognostic factors, and with respect to patient survival.
MATERIALS AND METHODS
Patients and tumours
All samples analysed were biopsies taken from patients with stage II–IIIa breast cancer and at least four involved lymph nodes (n = 66); the biopsies had been previously fixed in formalin and preserved in paraffin wax in the course of routine pathological assessment. All patients were entered into the Anglo Celtic I trial, and randomised in equal numbers to two “arms”. Arm 1 received induction treatment, consisting of four cycles of Doxorubicin, followed by conventional CMF chemotherapy. Arm 2 received the same induction treatment, followed by high dose cyclophosphamide and subsequent bone marrow transplantation. The particular patient subgroup of those entered into the Anglo Celtic I trial comprised those who were managed at the Northern Centre for Cancer Treatment, Newcastle General Hospital, Newcastle, UK.
For each patient, data were available concerning patient survival (including times to relapse and/or death). Also available were data describing tumour grade, tumour size, the proportion of involved nodes, and the presence of vascular invasion for each patient.
Assessment of antigen expression by immunohistochemistry
Immunohistochemistry was carried out using an indirect streptavidin–avidin biotin complex method. Briefly, sections were dewaxed and hydrated before blocking of endogenous peroxide using methanol/hydrogen peroxide. Antigen retrieval was carried out at high temperature and pressure using citrate buffer (200mM citric acid, 500mM NaOH, pH 6.0). Sections were then washed in 1× Tris buffered saline (TBS; 140mM NaCl, 50mM Tris/HCl, pH 7.6) and blocked using 20% normal rabbit serum (NRS) (in 1× TBS) for 10 minutes, before incubation with the primary antibody solution for one hour (table 1 lists the primary antibodies used and their dilution factors). After washing in TBS, sections were incubated with biotinylated rabbit antimouse secondary antibody (Dako, Ely, Cambridgeshire, UK) at a 1/500 dilution (in 20% NRS) for 30 minutes. After further washing, streptavidin–biotin (Dako) was added at a 1/100 dilution (in 20% NRS), and the sections incubated for 30 minutes. The final reaction was visualised using 3,3′-diaminobenzidine (Sigma, Poole, Dorset, UK) in a TBS/hydrogen peroxide solution for three minutes. Finally, sections were counterstained using Harris’s haematoxylin before being blued, and then dehydrated and mounted in DPX.
Antibodies used in immunohistochemical assessment of type 1 growth factor hormones and steroid hormone receptors
T1GFR status was assessed according to membrane and cytoplasmic expression, with the exception of c-erbB-4, which was assessed according to cytoplasmic and nuclear expression (essentially, no membrane staining was seen). The ER and progesterone receptor (PGR) were assessed according to nuclear expression. Evaluation of immunohistochemical staining was carried out by two histopathologists. Each estimated the proportion of tumour cells staining, and the average intensity of staining for the whole slide. Staining intensity was assigned a value of either 0 (negative), 1 (weak positive), 2 (intermediate positive), or 3 (strong positive). An average of the results for the two histopathologists was then taken. Cases in which the scores were discrepant by more than 10% (positive cells) or ⩾ 1 (intensity) were discussed using a conference microscope, and a value agreed. For each patient, the data were then combined to yield a final value reflecting both the proportion of positive cells and the intensity of staining. This was carried out according to the method of Detre,20 to yield a value between 0 (completely negative) and 18 (very strong positive). The data were classed as continuous for the purpose of statistical analysis.
Statistical analysis
To assess the relations between variables, two statistical tests were applied. Inter-relations between the molecular antigenic variables (T1GFRs, ER, and PGR (continuous data)) were assessed using Spearman’s test for rank correlations (bivariate). Further analysis was carried out after categorisation of continuous variables into two groups (high and low). The cut off value for the T1GFRs was the median value, and for ER and PGR, the cut off for positivity was a Detre value of greater than 2.20 Subsequent comparison with tumour grade, size, nodal involvement, and vascular invasion (categorical data) was then carried out using Fisher’s exact test. With the data in this categorical form, survival analysis was also carried out with respect to each variable. Kaplan Meier step graphs were constructed and survival analysis was carried out using the logrank test. All analysis was carried out using SPSS statistical software.
RESULTS
General statistics
Of the 66 patients examined, five patients had grade 1 tumours, 15 grade 2, and 46 patients grade 3. All patients had involved nodes, ranging from 18% to 100% of nodes examined, with a mean of 69.6%. Tumour diameter ranged from 0.9 to 8 cm, with a mean of 3.24 cm. Of the 66 patients examined, 39 patients had vascular involvement, whereas 23 did not. Regarding menopausal status, 43 patients were premenopausal, eight patients were perimenopausal, and 15 were postmenopausal. Thirty eight patients were assessed as ER positive (Detre score, > 2) and 38 were assessed as PGR positive (Detre score, > 2).
Expression of type 1 growth factor receptors
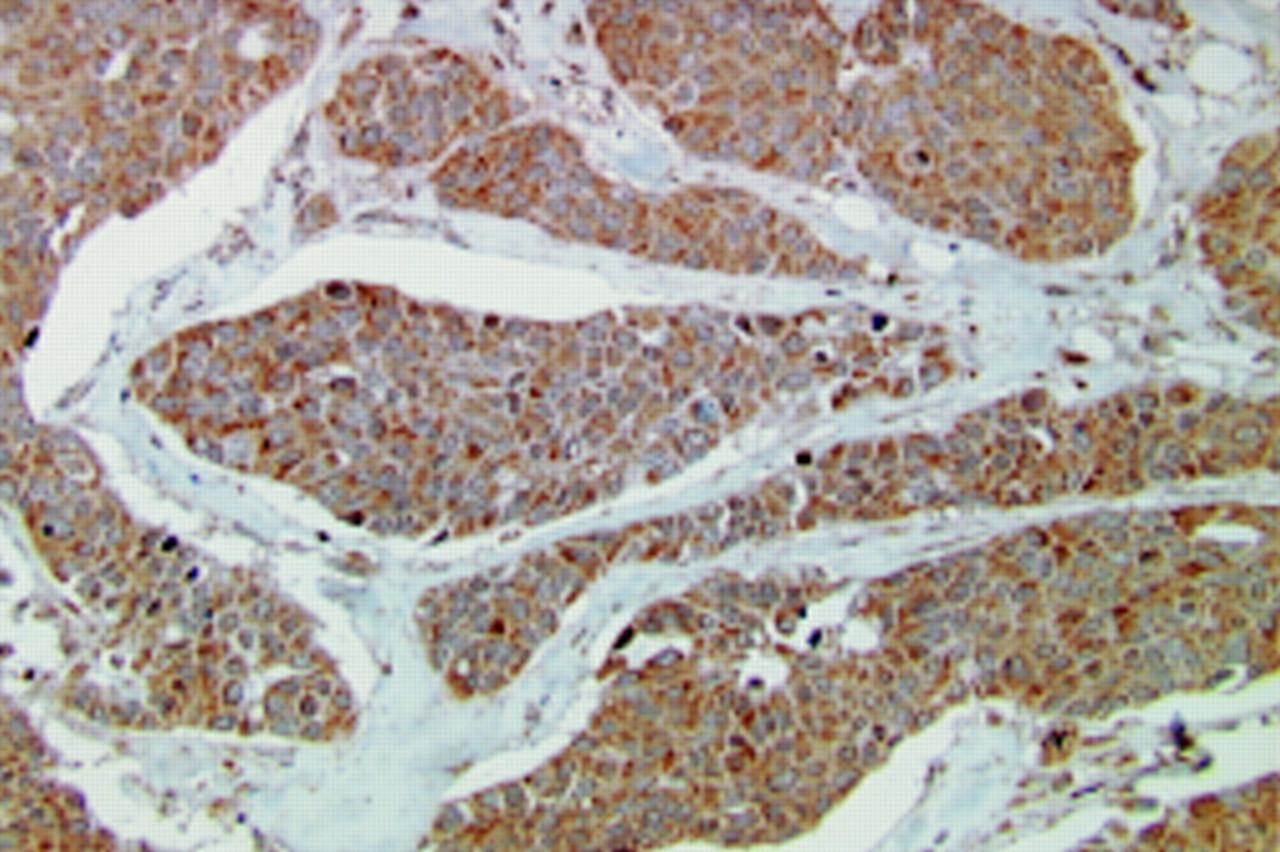
Immunostaining for EGFR, c-erbB-2, and c-erbB-3 was both membranous and cytoplasmic, whereas labelling for c-erbB4 was cytoplasmic and sometimes also nuclear, as described below. With regard to the expression of individual T1GFRs, the assessment of EGFR membrane staining showed 44 patients with some degree of staining (Detre score, > 0), and the median Detre score was 2. Fifty eight samples showed some cytoplasmic staining (median value, 5). With respect to c-erbB-2 staining, 64 patients showed some membrane staining (median value, 6) and 65 showed some cytoplasmic staining (median value, 6). Analysis of c-erbB-3 expression revealed that 48 (median value, 2) and 60 (median value, 5) patients had some degree of membrane and cytoplasmic staining, respectively. Regarding c-erbB-4 cytoplasmic expression, 61 cases showed cytoplasmic labelling (median value 6; fig 1), whereas 56 showed a degree of nuclear staining (median value, 2).

Immunohistochemical staining for c-erbB-4 showing cytoplasmic reactivity in tumour cells.
For c-erbB-2, the criteria for overexpression when assessed by immunohistochemistry is generally classed as being intermediate to strong membrane staining in > 10% of tumour cells (Dako Herceptest™). We did not use this cut off value in our statistical analysis, but purely as a comparative statistic, we found that 34 of the 66 patients overexpressed c-erbB-2 when assessed in this way. This is consistent with other studies, given that we have a high proportion of grade 3 tumours.16
Associations between variables
With regard to associations between the molecular antigenic variables assessed using Spearman’s test, positive associations were found between c-erbB-3 and c-erbB-4 cytoplasmic expression (p = 0.003). As expected, ER and PGR expression showed a significant correlation (p < 0.001). Negative associations were found between EGFR membrane expression and both ER (p = 0.001) and PGR (p = 0.023) expression.
With regard to additional assessment carried out after categorising the above variables into high and low groups (about the median) and comparison of the molecular variables with grade, tumour size, nodal involvement, and vascular invasion, a positive association was seen between EGFR membrane staining and tumour grade (p = 0.025). No other significant associations were found.
Survival analysis
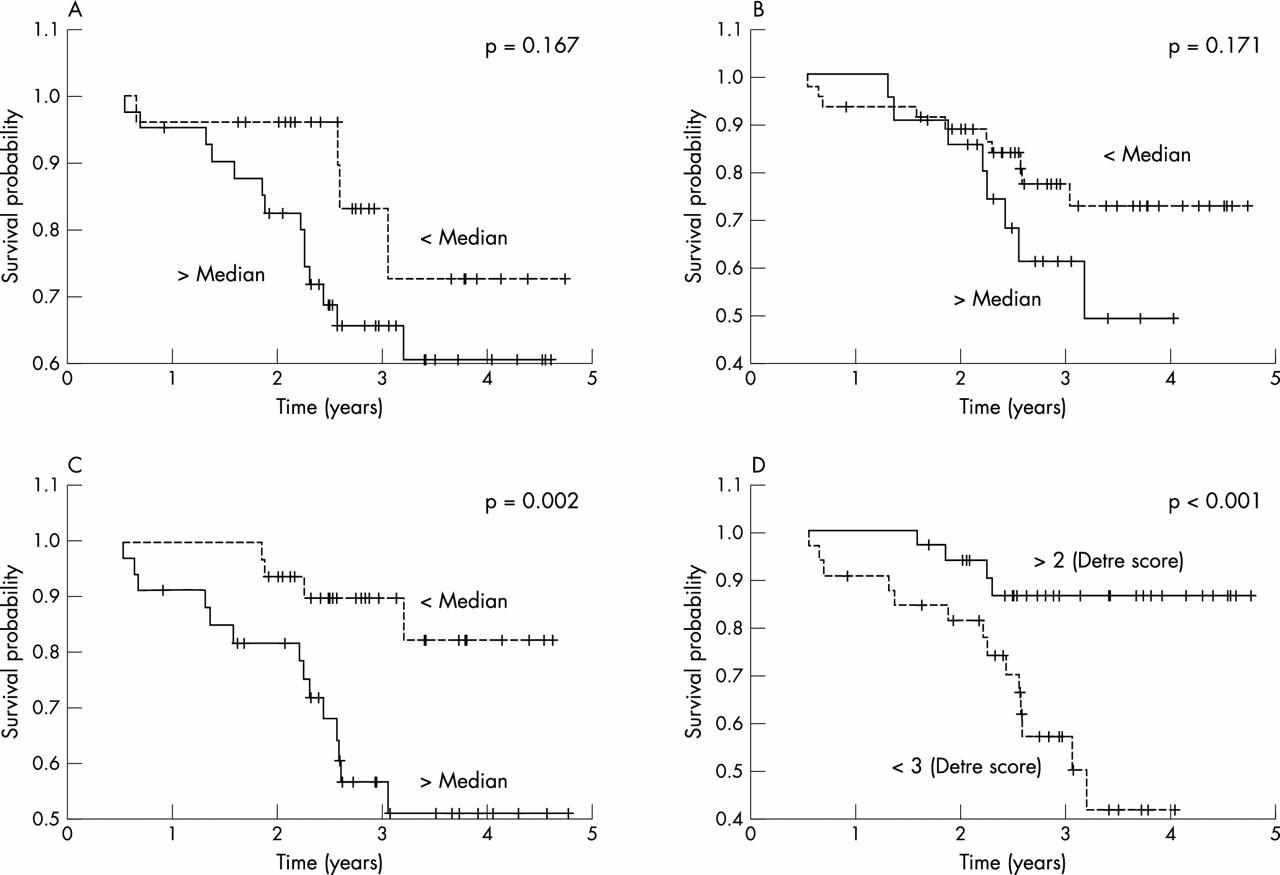
Survival analysis was carried out with respect to each variable. We found that high tumour grade and size were associated with poor survival, although significance was not quite reached. ER and PGR expression were both associated with improved survival, with ER reaching significance (p < 0.001; fig 2D). Of the T1GFRs, both EGFR and c-erbB-2 cytoplasmic expression were associated with poor survival, but the results did not reach significance (p = 0.167 and p = 0.171, respectively; fig 2A,B). c-erbB-3 expression showed no association with survival. However, upon analysis of c-erbB-4, patients with high cytoplasmic expression were found to fare significantly worse than those with low expression (p = 0.002; fig 2C).

{kind=link}
{kind=link}
Kaplan Meier step graphs showing survival analysis for (A) epidermal growth factor receptor cytoplasmic staining, (B) c-erbB-2 cytoplasmic staining, (C) c-erbB-4 cytoplasmic staining, and (D) oestrogen receptor (ER) nuclear staining.
DISCUSSION
In our study, despite the small number of patients studied, we have observed several established trends. First, the negative association seen between ER and EGFR expression (p = 0.001) is now well documented.17 Second, the survival trend observed with respect to ER expression (p < 0.001) is also well established.18
Regarding the T1GFR family, as stated previously, c-erbB-2 expression has been well characterised, and expression is known to be associated with a poor prognosis in breast cancer. Our results are consistent with this, although the result was not significant (p = 0.171). Concerning EGFR, our results showed a non-significant advantage for patients expressing low amounts of this receptor (p = 0.167). This result is in agreement with many previous studies.2,9,10
Very little information exists with respect to the prognostic implications of c-erbB-3 and c-erbB-4 expression. A large study of c-erbB-3 expression and its association with clinical outcome was performed by Travis et al.11 This study of 501 patients with breast cancer showed that 15% and 35% of patients with primary operable and advanced disease, respectively, had increased expression relative to normal tissue. However, no association with survival was found. Other studies by Lemoine and colleagues12 and Quinn and colleagues13 showed no significant relation between c-erbB-3 expression and survival, and our results are also consistent with these findings.
We found that patients expressing high amounts of cytoplasmic c-erbB-4 fared significantly worse that those expressing low amounts (p = 0.002). To our knowledge, this association has not been seen before. In a previous clinical study performed by Kew and colleagues14 no association between c-erbB-4 expression and survival was demonstrated in a study of 127 cases of breast cancer. The scoring system used was different from that used in our study because the proportion of positive cells was not taken into account, but rather a system based on average intensity was used. In addition, a heterogenous patient group was studied (for example, node positive and node negative patients, with treatment differences), whereas in our study we have investigated node positive patients with one or two treatment strategies entered into a clinical trial. Another clinical study by Srinivasan et al found no association between nuclear c-erbB-4 expression and patient survival.15 Knowlden et al found that c-erbB-4 protein expression was associated with a prognostically favourable ER positive phenotype,18 and using the reverse transcription polymerase chain reaction for c-erbB4 mRNA, Suo et al also found an association with positive ER status.17 Pawlowski and colleagues19 also found an association between c-erbB-4 mRNA values and ER, in addition to a significant association with better prognosis; these observations may again relate to the patients studied and the methods of assessment.
“Our results are largely consistent with previous studies, but our observation of an association between c-erbB-4 and poor prognosis is new”
The observed nuclear expression of c-erbB-4 was unexpected on the basis of current models of how growth factor receptors function, but has been noted previously by other authors.14 Experiments are currently under way using methods with higher resolution than immunocytochemical staining to determine whether this represents genuine intranuclear staining or perinuclear localisation.
We also found several additional associations between variables. First, we found a positive association between c-erbB-3 and c-erbB-4 cytoplasmic expression (p = 0.003). This may reflect a preferred heterodimerisation partnership in some cancers, although the cell membrane is the actual site for dimerisation. In addition, we found that EGFR expression was positively associated with tumour grade (p = 0.025). This is consistent with the fact that high EGFR expression and high grade are both associated with poor prognosis.
Take home messages
-
Overexpression of epidermal growth factor receptor, c-erbB-2, and c-erbB-4 was associated with adverse clinical outcome, although this was significant only for c-erbB-4
-
Although patient numbers are small, to our knowledge, this is the first report describing c-erbB-4 as an adverse prognostic marker, perhaps because all the patients studied had advanced stage disease and had undergone similar chemotherapy regimens in the context of a clinical trial
-
Thus, c-erbB-4 may be useful as a prognostic indicator in breast cancer and may also represent a new target for anticancer treatment in a similar manner to c-erbB-2 targeting by Herceptin®. Further investigations involving larger numbers of patients, including node negative patients, are warranted
We acknowledge that our study has certain drawbacks, the most obvious of which is the small number of patients examined, although the series is relatively homogeneous. Despite this, however, we have demonstrated several established trends, which help to strengthen our observations. Our results are largely consistent with previous studies, but our observation of an association between c-erbB-4 and poor prognosis is new. The strength of the association suggests that the trend may well be genuine. If so, c-erbB-4 may be useful as a prognostic indicator in breast cancer, identifying those patients in whom alternative or more aggressive treatment may be more effective, at least in the node positive group. It may also represent a new target for anticancer treatment in a similar manner to c-erbB-2 targeting by Herceptin®.5 There is evidence to suggest that c-erbB-2 may predict response to anthracycline treatment,21 and one study in non-small cell lung cancer showed that c-erbB-4 may predict the response to gemcitabine-cisplatin22; the role of c-erbB-4 as a predictive factor in breast cancer needs to be explored. Further investigations involving larger numbers of patients, including node negative patients, are clearly warranted. In these studies, it may be of value to investigate the significance not only of the expression of growth factors individually, but also to examine the profile of expression—for example, coexpression of c-erbB-2 with one or more heterodimerisation partners.
Acknowledgments
We are grateful to Amgen Ltd for their generous financial support.
REFERENCES
Footnotes
-
R C F Leonard represents the Anglo Celtic Co-operative Oncology Group